




The intravesical instilation of bacillus Calmette-Guérin (BCG) is a widely used and efficacious procedure for treatment of intermediate to high-grade superficial bladder cancer. The occurrence of osteoarticular side effects is infrequent compared to the number of administrated doses, and reactive arthritis is included within these effects. We present the case of a 54 years old HLA-27 (+) male, who developed reactive arthritis featuring asymmetric olygoarthritis and dactylitis after the second intravesical BCG instillation, which was resolved with administration of Etoricoxib and Isoniazid.
La instilación intravesical de bacilo de Calmette-Guérin (BCG) es un procedimiento ampliamente utilizado y eficaz para el tratamiento del carcinoma vesical superficial de grado intermedio y alto. La aparición de efectos colaterales osteoarticulares es infrecuente comparado con el número de dosis administradas, y dentro de estos se incluye la artritis reactiva. Presentamos el caso de un paciente varón de 54 años, HLA B27 (+), que desarrolló un cuadro de artritis reactiva caracterizado por oligoartritis asimétrica y dactilitis tras la segunda instilación intravesical de BCG, y que se resolvió con el tratamiento con etoricoxib e isoniazida.
Local immunotherapy by intravesical instillations of the Calmette-Guerin bacillus (BCG) has been used since 1976 in patients with intermediate and high grade superficial bladder carcinoma, its use being widespread at present and having proven safe and effective.1 Its antitumor activity is concentrated at the site of instillation, suggesting that the immunomodulatory activity is mainly local. However, this treatment is capable of inducing non-serious systemic side effects and self-limiting malaise and fever in up to 5% of patients.1,2 Osteoarticular side effects are rare, being described in 1%–5%, mainly joint pain and arthritis in 0.5%–1% of patients.3,4 We report the case of a patient who, after receiving 2 intravesical instillations of BCG for the treatment of bladder carcinoma, developed reactive arthritis (ReA).
Clinical PresentationThe case is a 54-year-old male, diagnosed in April 2010 with high grade superficial bladder carcinoma (stage pT1aG3), without systemic dissemination, treated with transurethral bladder resection and subsequently being programmed for the administration of 6 intravesical instillations of BCG with intervals of 15 days between June and August 2010.
After the second instillation, he began to show diffuse swelling and inflammatory pain of the second right toe compatible with dactylitis, and a few days presenting a similar episode on the third finger of his left hand. The right knee and left ankle were subsequently swollen (Fig. 1). Coinciding with the joint manifestations, the patient developed fever (up 38.8°C, without associated dysthermia), purulent urethral discharge and self-limiting diarrhea during the first 2 days. He did not present eye inflammation or skin lesions, and had no limitations or inflammatory signs of the axial skeleton or entheses. The patient denied similar previous episodes of arthritis, back pain or history of inflammatory or heel pain, but had a family history of spondyloarthritis (a brother with ankylosing spondylitis [AS]).

From the analytical point of view, he showed an increase of acute phase reactants (C reactive protein98.60mg/l, erythrocyte sedimentation rate 97mm/l; first hour), with other tests resulting normal, including blood chemistry, CBC, immunology (rheumatoid factor, antinuclear antibody, complement and immunoglobulins) and serology (Chlamydia, Salmonella, Yersinia, Brucella, human immunodeficiency virus, hepatitis viruses B and C). The culture of the urethral discharge was also negative. HLA typing revealed the presence of A24/AX, B44, B27, BW4/BW4, DQ7 and DQ5.
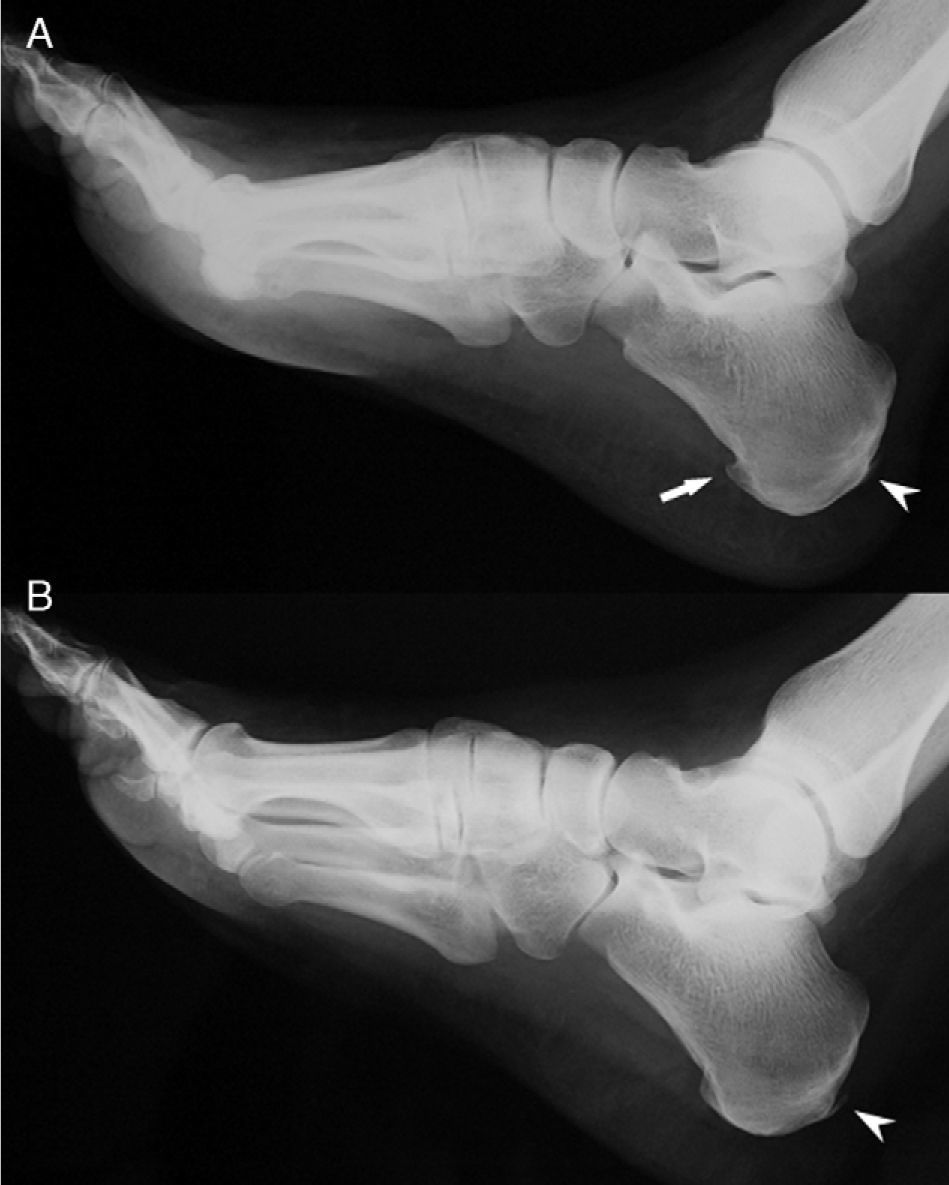
The radiographs of hands, feet, ankles and knees showed only soft tissue growth corresponding to arthritis without joint erosions, but entesophytes were identified on the Achilles tendon as well as a bilateral right heel spur (Fig. 2). Sacroiliac X-rays and MRI were normal. Doppler ultrasound detected signs of synovitis and tenosynovitis of the second PIP flexor tendon of the third finger of his left hand, second and third right metatarsophalangeal joints and second left tibiotalar joint as well as the right knee, with no increase in the power-Doppler signal.
Because of the temporal relationship between the intravesical BCG instillation and the onset of dactylitis and the asymmetrical oligoarthritis with urethritis, fever and HLA-B27 (+) with subclinical enthesopathy, we established the diagnosis of ReA secondary to BCG. The patient initially received low-dose corticosteroids (prednisone 5mg/day), without any improvement, so we associated etoricoxib 90mg/day and isoniazid 300mg/day, with treatment lasting up to 4 months, between October 2010 and February 2011, achieving progressive control and complete disappearance of the inflammatory joint signs in 3 months. After 6 months no joint remission (or axial or peripheral) or other manifestations suggesting active disease have been seen.
DiscussionThe development of musculoskeletal side effects secondary to intravesical BCG instillation for the treatment of bladder cancer is very rare considering its wide distribution and the number of patients under treatment, reducing its frequency to case reports and small series.3 Tinazzi et al. conducted a systematic review of 48 articles that included 61 cases of autoimmune manifestations related to the intravesical administration of BCG. They found joint pain and/or arthritis in 64% of patients, Reiter's syndrome in 24%, arthritis and fever in 4%, peripheral arthritis in patients with AD in 4%, psoriatic arthritis in 2% and Sjögren's syndrome in 2%.1
ReA secondary to BCG usually occurs in men between 50 and 60 years of age, manifesting as asymmetric and additive arthritis, normally found in knees, ankles and wrists, and fever associated in more than half of cases.5 Dactylitis,6 urethritis8 and uveitis7 have also been described as part of this picture. Most often it develops late after the fourth or fifth instillation (although in our case it appeared after the second). In complementary examinations there is usually a moderate increase in acute phase reactants, joint fluid has inflammatory characteristics with predominance of polymorphonuclear cells and mycobacteria cultures obtained from the joint fluid, urine and blood are negative (thus excluding the possibility of septic arthritis by BCG, which has also been described).3,5
The mechanism by which the instillation of BCG induces ReA is not established. It has been suggested that molecular mimicry could be a cause, because the heat shock protein HSP65 of mycobacteria shares homology with a human cartilage proteoglycan, and also presents cross-reactivity with the haplotypes of HLA-DR1, DR3 and DR4, stimulating the secretion of cytokines and activation of CD8 (+).9 The autoimmune response induced by the administration of BCG occurs more frequently in patients with HLA-B27 (+) (nearly 60% of reported cases) or B7 (+) (which shows strong affinity with HLA-B27).1
Most patients with secondary ReA respond favorably to complete suspension of BCG treatment. The disease may become chronic in a small percentage of cases and requires specific therapy, with NSAIDs and corticosteroids used alone or in combination, rarely requiring the association of immunosuppressants such as methotrexate. In patients with an inadequate response to these treatments, as in our case, some authors suggest the addition of anti TB drug treatment.1 Although this approach is controversial, some chronic and refractory cases have been reported solved after treatment with isoniazid for 3 months.10,11
ConclusionsThe development of ReA following intravesical BCG immunotherapy in patients with bladder carcinoma is a rare event. However, we should consider this diagnosis when confronted with an osteoarticular clinical picture in patients treated with BCG. It is more common in patients with HLA B27 and B7, and generally has a self-limited course and a favorable prognosis.
Ethical disclosuresProtection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of Data. The authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consent. The authors have obtained the informed consent of the patients and /or subjects mentioned in the article. The author for correspondence is in possession of this document.
Conflict of InterestThe authors have no disclosures to make.
Please, cite this article as: Macía Villa C, et al. Artritis reactiva secundaria a la instilación intravesical de bacilo de Calmette-Guérin. Reumatol Clin. 2012. doi:10.1016/j.reuma.2011.11.009


