




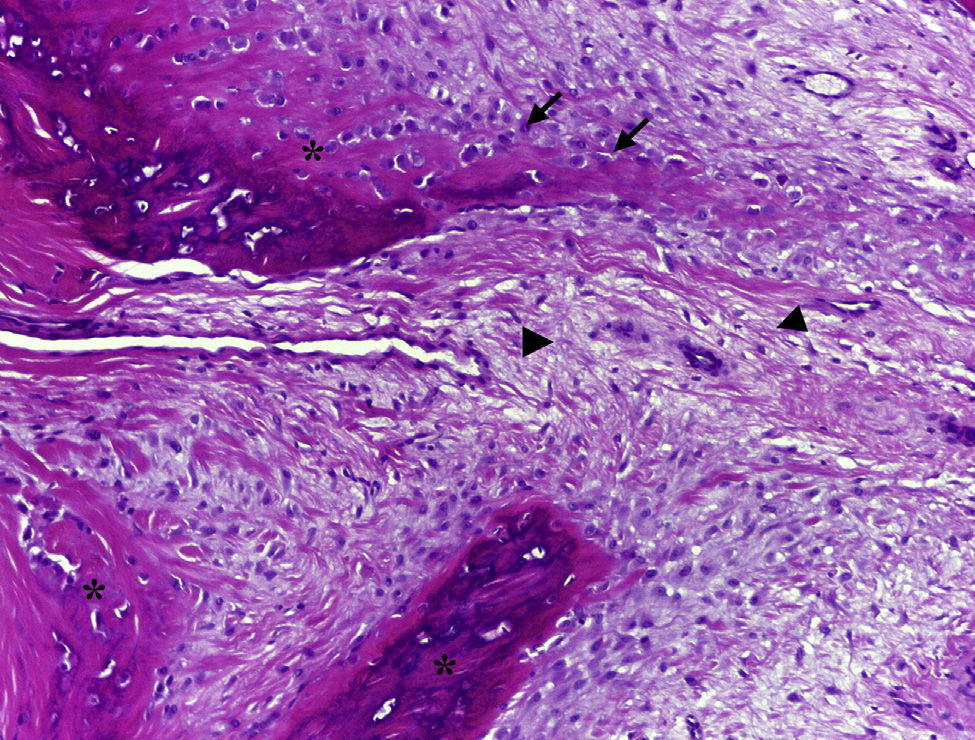
The patient is a 29-year-old woman, who complains of swelling and pain in the fifth finger of the left hand lasting for 3 months. She had no medical history and no previous trauma of the referred finger. On examination, she presented a tumor of 1.5cm×0.5cm on the tip of the finger and the subungual region, of indurated consistency which adhered to deep planes, with mild erythema and tenderness. Radiological studies showed a well-circumscribed, nodular ossified lesion with irregular borders, adhered to the l periosteum of the distal phalanx, without erosion of the cortex (Fig. 1). Laboratory studies, including biochemistry, hematology and acute phase reactants were all normal. Excision of the lesion was performed and the histopathological study revealed fibrous tissue and fibroblasts with prominent nuclei without atypia in its periphery, and immature osteoid deposits surrounded by an osteoblastic rim in the central area (Fig. 2). These findings were consistent with the diagnosis of florid reactive periostitis of the hand (FRPH). There was no recurrence of the lesion.

FRPH is a rare benign entity characterized by a lush production of osteoblastic proliferative fibrous stroma in the periosteum of the fingers.1 Its pathogenesis is unknown but is considered to correspond more to a reactive process than to a neoplasm, with a history of trauma being present in up to 50% of cases.2 Although it was described in 19333 there still is confusion in the literature caused by different denominations, including paraostal fasciitis, ossifying fasciitis, fibro-osseous pseudotumor, pseudomalignant bone tumor of the soft tissue of the fingers and nodular fasciitis, with FRPH being the accepted term.2,4 It is most frequently located in the proximal phalanx, followed by the middle phalanx, metacarpal joints and distal phalanx; it is rare in the first two fingers. It usually occurs in women during the second and third decades of life, and is clinically characterized by swelling, pain and erythema of the affected finger.2,5 Radiographs show increased soft tissue and periosteal new bone formation, which may have a lamellar or mature bone5 appearance. The cortex is usually intact, although erosions have been occasionally described.6 The differential diagnosis includes infections (septic tenosynovitis, soft tissue abscess with bone involvement, cortical osteomyelitis), myositis ossificans, benign tumors such as giant cell tendon sheath tumors and osteochondroma, and malignant ones such as the paraostal and periosteal osteosarcoma, synovial sarcoma and periosteal chondrosarcoma.1,5 The recommended treatment is local excision, which is curative in most cases.5 In conclusion, although FRPH is an uncommon lesion, it should be taken into account because it can simulate other more serious conditions such as malignant bone neoplasms.
Ethical ResponsibilitiesProtection of people and animalsThe authors declare that no experiments have been performed on humans or animals.
Data confidentialityThe authors declare that they have followed the protocols of their workplace regarding the publication of data from patients and that all patients included in the study have received sufficient information and have given their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained informed patients and/or subjects referred to in the article. This document is in the possession of the corresponding author.
Conflict of InterestThe authors declare no conflicts of interest.
Please cite this article as: Blázquez Cañamero MÁ, et al. Periostitis reactiva florida de la mano. Reumatol Clin. 2014;10:262–263.


