
Right ventriculoarterial coupling (RVAC) is altered early before presenting right ventricular dysfunction and pulmonary hypertension, its measurement in patients with RA has been barely studied.
ObjectivesTo determine if there is a difference in right ventricular arterial coupling (RVAC) in patients with RA. Analyze if there are differences in patients with normal vs abnormal right RVAC. To investigate if there is an association in patients with RA to present abnormal RVAC.
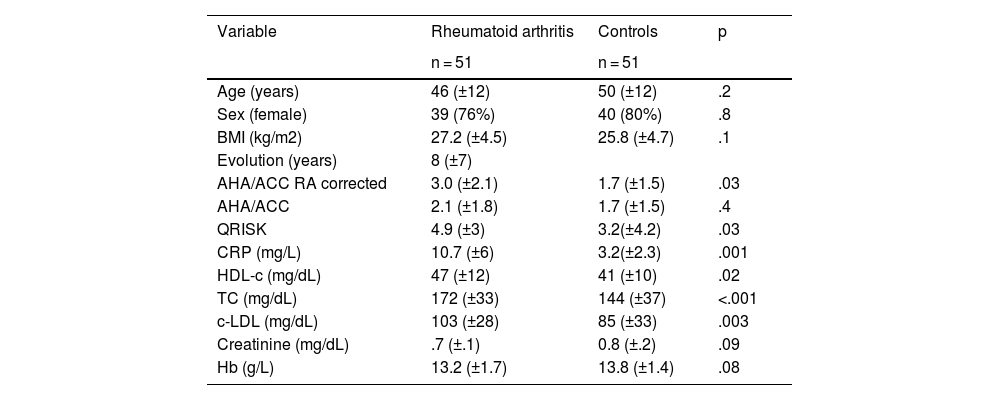
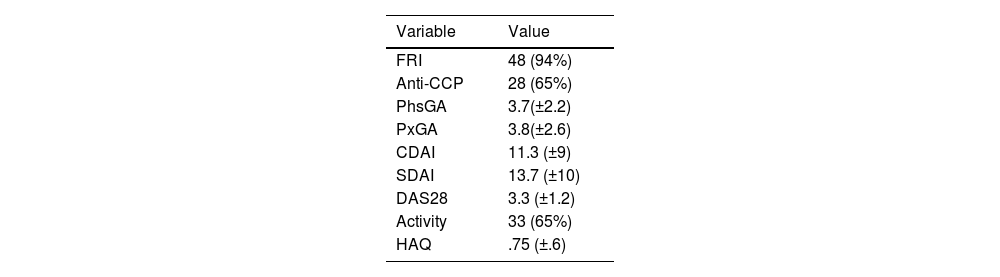
MethodsA single-center, analytical, cross-sectional, observational study was performed. Patients with a diagnosis of RA were included according to the ACR/EULAR 2010 classification criteria, without any other comorbidity, the echocardiograms were made at the Hospital Civil de Guadalajara “Fray Antonio Alcalde”. An ACUSON SC 2000 echocardiogram was used. Patients were compared with healthy controls matched by age and gender. The clinical, laboratory and echocardiographic variables were contrasted. The RVAC was determined with the right ventricular free wall longitudinal strain (RVFWLS) / pulmonary artery systolic pressure (PSAP) ratio.
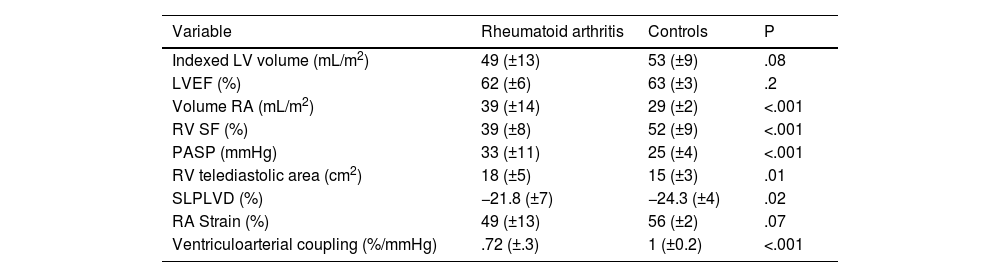
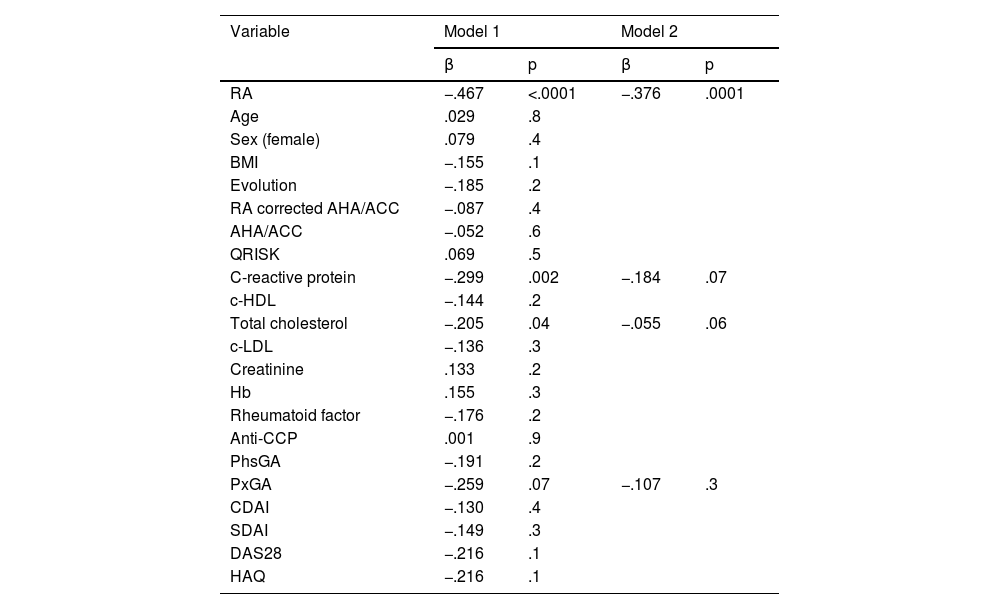
ResultsFifty one patients were included in each group. Among the echocardiographic variables, it was found that patients with RA had a greater right ventricular diastolic area and the PASP; while the RV FAC, the RVFWLS and the RVAC were lower. RA was independently associated to an abnormal RVAC.
ConclusionThe right ventricular subclinical myocardial damage, determined by the RVAC, is present in patients with rheumatoid arthritis, and it was associated with an abnormal ventriculoarterial coupling.
El acoplamiento ventriculoarterial derecho puede alterarse precozmente antes de presentar disfunción del ventrículo derecho e hipertensión pulmonar, su medición en pacientes con Artritis Reumatoide ha sido poco estudiado.
ObjetivosDeterminar si existe diferencia en el acoplamiento ventriculoarterial derecho en pacientes con AR. Investigar si existe la asociación en pacientes con AR para presentar acoplamiento ventriculoarterial anormal.
MétodosSe realizó un estudio unicéntrico, analítico, transversal, observacional. Se incluyeron los pacientes con diagnóstico de AR según los criterios de clasificación de la ACR/EULAR 2010, sin ninguna otra comorbilidad, que se les realizó un ecocardiograma en el Hospital Civil de Guadalajara “Fray Antonio Alcalde”. Se compararon los pacientes con controles sanos pareados por edad y género. Se contrastaron las variables clínicas, de laboratorio y ecocardiográficas. El acoplamiento ventriculoarterial derecho se determinó con la relación strain de la pared libre del ventrículo derecho (SLPLVD)/presión sistólica de arteria pulmonar (PSAP).
ResultadosSe incluyeron 51 pacientes en cada grupo. Dentro de las variables ecocardiográficas, se encontró que los pacientes con AR tenían mayor área telediastólica del VD, la PSAP; mientras que fue menor la FAC VD, el SLPLVD y el AVAD. Se asoció que el padecer AR era un factor asociado de manera independiente a la disminución del AVAD.
ConclusiónEl daño miocárdico subclínico del ventrículo derecho, determinado por el acoplamiento ventriculoarterial, está presente en los pacientes con Artritis reumatoide. El padecer artritis reumatoide se asociaron a presentar un acoplamiento ventriculoarterial anormal.



