

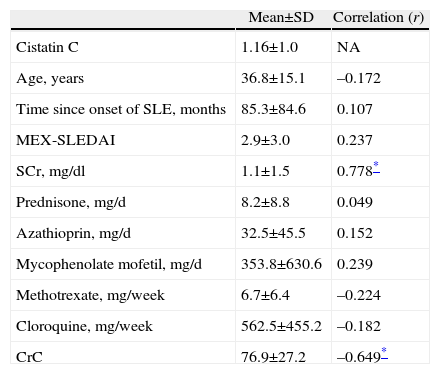
Kidney damage occurs in more than half of patients with systemic lupus erythematosus (SLE).1 The glomerular filtration rate (GFR) is the most important marker of renal function and crucial for diagnosis, stratification and response to treatment.2 The ideal marker of GFR should be constantly produced, be freely filtered, not reabsorbed or secreted by the renal tubules or metabolized or eliminated by extrarenal mechanisms.2 Inulin meets these characteristics, however, the measurement of GFR by this method is very complex, expensive and difficult to perform.3 The surrogate marker employed is endogenous creatinine, which does not complete the requirements of an ideal marker because it is subjected to tubular secretion as well as being influenced by the muscle mass of the patient.2 Cystatin C is a protein produced by all nucleated cells, freely filtered by the glomerulus, not returned to the bloodstream and not secreted by the renal tubules.2,4 The above features make it a better marker of renal function than creatinine,5 however, we recognize that there are different factors influencing the levels of cystatin C to be taken into account when performing this test, such as levels of C reactive protein, smoking, obesity, gender, glucocorticoids, age and diabetes.6,7 Based on the above, this test could be useful to assess renal function in patients with lupus nephritis (LN) in whom various factors associated with both disease (lupus) and the drugs used could modify the levels of cystatin C.8 We included 60 consecutive patients with SLE in the order in which the blood sample was taken to determine levels of creatinine (creatinine standardized by the Roche enzymatic method) and cystatin C (immunonephelometric test particles). Table 1 shows the mean±standard deviation (SD) of the data evaluated in patients, as well as the correlation (Pearson's rho) that existed between cystatin C and the different factors.
Characteristics of 60 Evaluated Patients.
| Mean±SD | Correlation (r) | |
| Cistatin C | 1.16±1.0 | NA |
| Age, years | 36.8±15.1 | –0.172 |
| Time since onset of SLE, months | 85.3±84.6 | 0.107 |
| MEX-SLEDAI | 2.9±3.0 | 0.237 |
| SCr, mg/dl | 1.1±1.5 | 0.778* |
| Prednisone, mg/d | 8.2±8.8 | 0.049 |
| Azathioprin, mg/d | 32.5±45.5 | 0.152 |
| Mycophenolate mofetil, mg/d | 353.8±630.6 | 0.239 |
| Methotrexate, mg/week | 6.7±6.4 | –0.224 |
| Cloroquine, mg/week | 562.5±455.2 | –0.182 |
| CrC | 76.9±27.2 | –0.649* |
SD, standard deviation; SCr, serum creatinine; CrC, creatinine clearance; MEX-SLEDAI, Mexican Systemic Lupus Erythematosus Disease Activity Index.
We included 5 pediatric patients and 55 (91.7%) were women, 63.3% used prednisone at the time of determination, 36.7% azathioprine, 28.3% mycophenolate mofetil, 53.3% methotrexate, 58.3% chloroquine and 73.3% statins. The correlations that showed statistical significance were creatinine and creatinine clearance. The importance of negative results (no correlation) implies that cystatin C may be a good marker of renal function in patients with lupus nephritis, since factors such as disease activity or use of drugs such as glucocorticoids do not modify the renal levels of this marker. On the other hand, it is necessary that studies determine the best equation to determine GFR in patients with LN, as there are different equations for patients with diabetes or chronic kidney disease, but not for rheumatic disease, which have different implications for renal9 damage10. Another important point to consider when estimating renal function is the cost of the test in our country (Mexico), which is on average $30 (U.S.), a cost 2.5 times greater than creatinine clearance and 8.5 times the creatinine determination only.
FinancingThis study was partially funded by the Mexican College of Rheumatology with 35000 pesos (2500 U.S. dollars approximately).
Please cite this article as: Martínez-Martínez MU, Abud-Mendoza C. Cistatina C sérica como marcador de función renal en pacientes con lupus eritematoso sistémico. Reumatol Clin. 2012;8:158–61.


