





The patient was an 85-year-old man with a history of hypertension, dyslipidemia and ischemic heart disease, who had undergone revascularization for unstable angina in 1985 by double coronary artery bypass. He received standard treatment con amlodipine, atorvastatin, pentoxifylline, telmisartan/hydrochlorothiazide, omeprazole, tramadol and acetylsalicylic acid. He was referred to rheumatology because of the suspicion of severe arthritis of right wrist, with no history of a traumatic injury (Fig. 1A). Physical examination revealed a soft tissue mass in the medial ulnar fossa. It was swollen, tender on palpation and mobile. The patient did not have fever, lymph node involvement or complain of changes in his general state. Bilateral radiographs of the hands confirmed diffuse osteopenia, narrowing of the carpal and midcarpal joint space and erosion of the distal ulna and of the styloids, as well as generalized vascular calcifications (Fig. 1B).
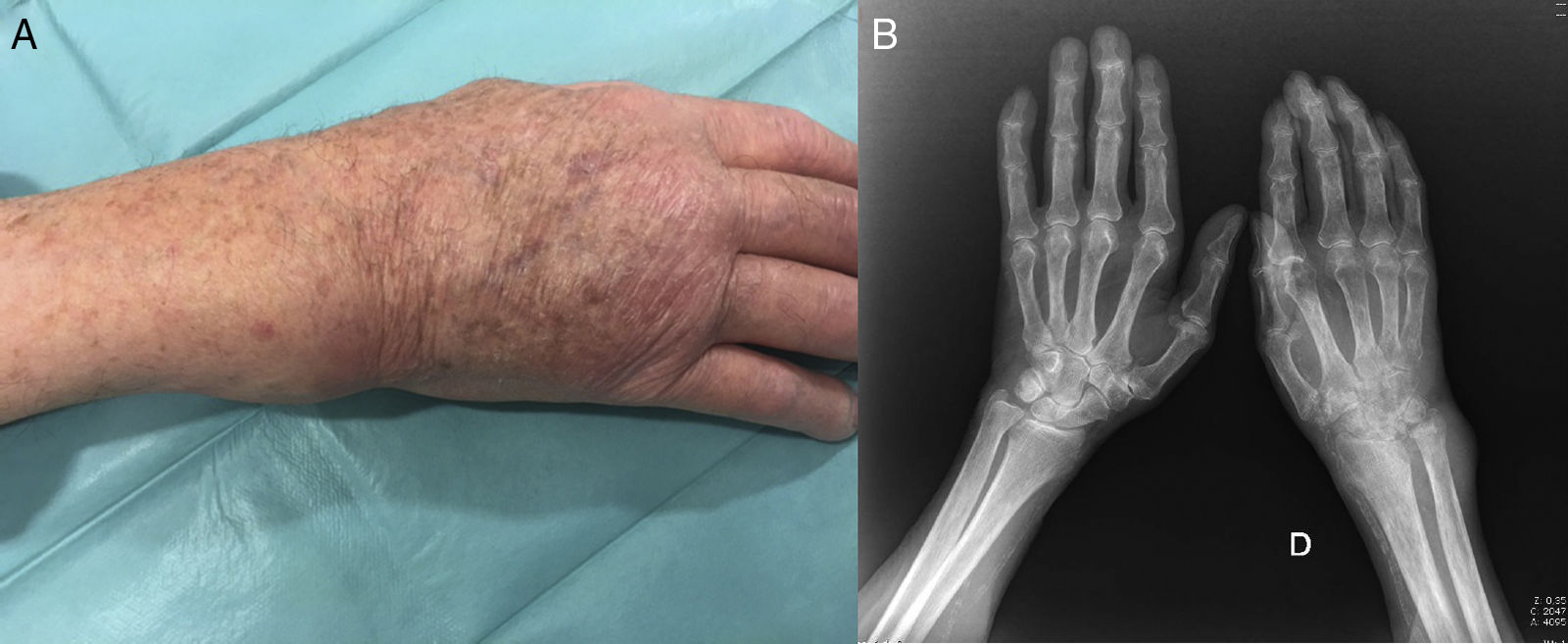
(A) Image of the patient's right wrist. Soft tissue mass located in the region of ulna that responded to pressure and was mobile. (B) Plain bilateral radiographs of the hands. Generalized osteopenia, reduction of the joint space in right wrist. Thickening of soft tissue most evident in the region of the ulnar styloid. Severe distortion of the architecture of the radiocarpal joint and ulnocarpal fossa.
We performed a gray-scale diagnostic ultrasound examination (Esaote MyLab 70®), which showed a round, defined, mobile cluster that extended in a heterogeneous manner throughout the 6 compartments of the extensor mechanism of the wrist (Fig. 2A). Color Doppler ultrasound revealed vascularization corresponding to G3, suggesting an active inflammatory-infectious process (Fig. 2B and C). Ultrasound-guided puncture yielded 5cc of cloudy fluid that, in direct Gram stain, showed abundant leukocytes, the absence of microorganisms and aerobic culture was negative. Ziehl–Neelsen stain disclosed no acid-fast bacilli either. However, after 9 days in Lowenstein–Jensen culture at 37°C, the existence of Mycobacterium tuberculosis was confirmed. A chest radiograph revealed a cardiothoracic index >0.5, sternal cerclage, minimal posterior strangulation of the costophrenic sinus, increase in right apical density, and tuberculostatic treatment was begun with 5 drugs (5 tablets of Rimstar®/day, together with oral vitamin B6/weekly, for 9 months), to treat infectious monoarthritis produced by M. tuberculosis.
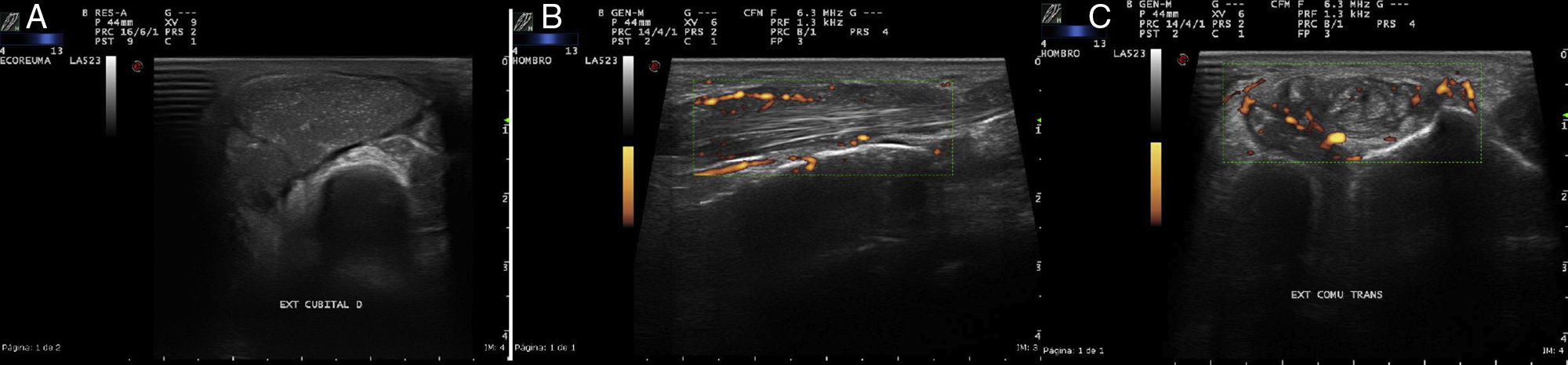
(A) Image of the dorsal compartment of right wrist. Distortion of the architecture of the extensor compartments. Presence of a large soft tissue mass that deforms the border of the common extensors, the extensor of the fifth finger and the extensor of the ulna. (B) Longitudinal view, and (C) transverse view of the common extensor tendon of the fingers at the level of the wrist. Increase in neovascularization with evident color Doppler signal (G3) showing activity over the extensor tendon and infiltration of surrounding infectious material.
Tuberculous infection continues to be a primary health care problem. Musculoskeletal involvement is encountered in between 10% and 15% of the patients with extrapulmonary tuberculosis.1 Arthritis and tenosynovitis of the wrist is underdiagnosed and the diagnosis is often delayed, a fact that is associated with a high worldwide mortality.2–4 Infectious arthritis affecting the wrist frequently develops in patients with an immunodeficiency.5 The diagnosis requires specific microbiological techniques and, as in this case, ultrasound-guided joint puncture enables direct diagnosis, ruling out other possible benign and malignant neoplastic diseases.6,7
In rheumatology, it is common to receive patients referred for the study of arthritis with no orientation or diagnostic tests. The present case is useful because: (1) it includes infectious arthritis due to M. tuberculosis in the differential diagnosis of monoarthritis of the wrist; (2) the ultrasound images lead to the suspicion of the severity of the disease, resulting in puncture and to the initiation of specific treatment; and (3) it points out the importance of access to rheumatological studies in the diagnosis of soft tissue masses and of the ultrasound findings for reaching a diagnostic and therapeutic decision. The accessibility of ultrasound and ultrasound-guided puncture were fundamental in the diagnosis.
Ethical DisclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of InterestThe authors declare they have no conflicts of interest.
Please cite this article as: Corominas H, Reina D, Torrente-Segarra V, Chico C, Antón V, Estrada P, et al. Idoneidad de la punción guiada por ecografía de alta resolución en el diagnóstico de una tumoración de partes blandas infectada por Mycobacterium tuberculosis. Reumatol Clin. 2018;14:171–172.
The present manuscript was written during a stay as a visiting faculty member in Beth Israel Medical Center, Harvard Medical School, in Boston, Massachusetts, United States, partially financed with a grant from the Catalan Society for Rheumatology (CSR).


