


Several generic questionnaires have been used to measure quality of life in patients with osteoarthritis (OA) since few instruments have been developed specifically for OA and none was developed for Spanish speaking patients. The purpose of the study was to validate and adapt to Spanish the French questionnaire AMICAL to measure quality of life in patients with hip and knee OA.
MethodsTransversal, analytical study. The validation process was performed in phases: translation from French to Spanish, translated version analysis by a multidisciplinary expert team, application of a pilot test to patients to evaluate grammatical and content equivalence, blind back translation, and analysis. The questionnaire was applied to hip and knee OA patients, together with the SF-36 questionnaire, as well as the WOMAC and the Lequesne indexes. The reproducibility was evaluated applying the questionnaire after 72h. The clinimetric analysis was calculated with SPSS 16.0.
ResultsOne hundred patients with hip OA and 100 patients with knee OA, radiological stages ii-iii, were included to evaluate homogeneity. Sixty-five patients with hip OA and 65 patients with knee OA were included to evaluate consistency. The final sample included 100 hip and 100 patients knee OA patients to estimate homogeneities and 65 patients were evaluated to estimate consistency. Mean (SD) age of patients with hip and knee OA was 56.34±13 and 60.1±9.2, respectively. Sixty seven percent and 79.8% were female, respectively. Cronbach’ alpha for AMICAL was 0.946 and 0.999, for hip OA and knee OA, respectively; and test-retest reliability using the intraclass correlation coefficients was 0.979 and 0.998, respectively. There was also a significant correlation with all the instruments (P<.05), except with the Lequesne index (r −0.383).
ConclusionsThe Spanish version of AMICAL questionnaire keeps the clinimetric properties, homogeneity, and consistency, and has a good correlation with other instruments. Consequently, it is reliable and self-applicable, and includes domains beyond the functional capacity that better evaluate the quality of life.
El impacto en la calidad de vida (CV) que condiciona la osteoartrosis (OA) ha sido evaluado con cuestionarios genéricos debido a que hay escasos instrumentos desarrollados específicamente para esta entidad y ninguno ha sido validado al español. El objetivo del estudio fue validar y transculturizar al español el cuestionario francés AMIQUAL para medir CV en pacientes con OA de caderas y rodilla.
MétodosEstudio transversal, analítico; el proceso de validación se llevó a cabo en las siguientes fases: traducción del francés al español, las versiones traducidas se analizaron con panel de expertos multidisciplinario, aplicación de prueba piloto en población con OA para valoración de equivalencia gramatical y de contenido, retrotraducción y análisis. Se validó en pacientes con OA de cadera y rodilla, junto con SF-36, así como índices de Womac y Lequesne. La reproducibilidad se evaluó aplicando el cuestionario a las 72h. El análisis clinimétrico se calculó con SPSS 16.0.
ResultadosSe incluyó a 100 pacientes para cada tipo de OA (cadera y rodilla), grado radiológico ii-iii, para estimar homogeneidad, y 65 pacientes para cada tipo de OA, para evaluar consistencia; la edad promedio fue de 56,34±13 y 60,1±9,2 años, respectivamente; predominó el género femenino, el 67% y el 79,8%, respectivamente. El α de Cronbach fue de 0,946 y 0,999 para OA de cadera y de rodilla, respectivamente; los coeficientes de correlación intraclase fueron 0,979 y 0,998, respectivamente. Las correlaciones con todos los instrumentos fueron significativas (p<0,05), excepto con el índice de Lequesne (r −0,383).
ConclusionesLa versión en español del cuestionario AMICAL conserva las propiedades clinimétricas, la homogeneidad y la consistencia, y correlaciona con otros instrumentos, por lo que es confiable, autoaplicable e incluye dominios más allá de la capacidad funcional, que interpretan mejor la CV.
The most prevalent rheumatic disease is osteoarthritis (OA),1,2 affecting at least 13.9% of adults from age 25 years and 33.6% of those over 65.3 OA of the knee is present in 16% of subjects from the age of 454 and 12.1% of those aged 65 years5; hip OA is reported in 4.4% of the population older than 55.2 In Mexico, the prevalence of OA is 10.5%, predominating in women.6 Its main manifestations are pain and stiffness, followed by limitation of motion, decreased strength and joint instability7,8 thus affecting functional capacity and causing a significant impact on quality of life (QOL) related to the state of health. QOL is considered a comprehensive indicator of the biopsychosocial role and is useful in the assessment of the patient situation and for making decisions about their management; however, there is no QOL tool in Spanish to evaluate these patients. Specific questionnaires of functional capacity, such as the WOMAC or Lequesne index, are limited to measure the specific impact on the QOL, because they are only partial assessments of this complex perception.1,8 On the other hand, it is known that the Spanish language is spoken by at least 500 million people in the world; therefore, it is the second most spoken European language and because of the migratory movement this frequency is increasing, so in countries like the United States it ranks fourth as the most spoken and is the second in Canada. In Brazil and EU countries such as Germany, France or Britain, there are millions of Spanish speakers. However, there are few validated instruments in Spanish to measure QoL in OA and those available are generic (e.g. SF-36), which determine loss of fidelity and specificity of information and monitoring after therapeutics,9–11 thus leading to the need for validated instruments specific to Spanish speakers. The AMIQUAL questionnaire is specific to assess QoL in patients with OA of the lower extremities; it was developed in France in 2005 and consists of 43 items, now in version 2.3, it is grouped into 5 domains: physical activity (19 items), mental health (14 items), social support (4 items), social functioning (3 items) and pain (3 items), plus 3 items related to family, sexuality and employment. Each item is answered on a simple scale of 1–10, with lower scores reflecting better QOL, the sense of the score is invested in questions 30–32, 39, 40, 42 and 43, so their interpretation can be quantified backwards; filling time takes approximately 11–15min.12,13 It has been validated and transculturized in different languages, demonstrating significant correlation coefficients (intraclass correlation coefficient [ICC] 0.70–0.85) with instruments such as SF-36 (r 0.43–0.75) and satisfactory discrimination, however, has not yet been validated in Spanish,14–17 so the objective of this study was to validate and AMICAL and transculturize the questionnaire as well as determine its correlation with other instruments. The authors of the original instrument in French, AMIQUAL, Francis Guillermin and Anne-Christine Rat, have provided authorization for the Spanish transculturization and validation of the questionnaire, and their respective use by the authors of this article.
Materials and MethodsA cross-sectional analytical study was conducted, in which the target population included adults with knee osteoarthritis and radiographic osteoarthritis of any degree, who accepted to participate under informed consent, of any gender and that excluded patients with cognitive impairment or previous neurological disorder that prevented the filling of questionnaires. Sampling of consecutive cases was non-probabilistic; the sample size was obtained by Epidat 3.1 software, by calculating the expected concordance, consistency and correlation, considering the sample size of its transculturation in other countries, the incidence of patients with osteoarthritis of the lower limbs of a rehabilitation unit and taking the specific QOL as the main variable. The study was submitted to the corresponding Local Committee for Research in Health according to the World Medical Association Declaration of Helsinki18 and the General Health Law, under informed consent.
TransculturationThe AMIQUAL 2.3 version questionnaire was translated by a bilingual professional with French as mother tongue, without medical knowledge, and a bilingual Spanish mother tongue health professional. Both versions were subjected to analysis by a multidisciplinary panel of 5 experts with at least 5 years of experience in the field of OA, which included: a nurse, a general practitioner or family doctor, a rehabilitation physician, a metrologist, a professional translator and a patient type. This analysis was blinded, independent and evaluated the grammar and content equivalence; it was confronted with the results of a pilot study of patients without OA, homogeneous in age and gender, and the final version was obtained by unanimous consent attaining a kappa of at least 0.80. The final version was submitted for reverse-translation by a teacher in bilingual French, with French as a mother tongue and a diagnosis of knee OA, and a bilingual professional Spanish mother tongue health professional, with final approval by unanimous agreement of linguistic equivalence made by the panel and the final name given to the instrument as Osteoarthritis of lower limbs and Quality of Life (AMICAL) (see Banexo Appendix 1).
ValidationTwo standardized interviewers were trained to perform the application of the instrument in interview mode for patients with less than six years of primary school (primary) and auto-filled mode for those with full-schooling and higher studies. The instruments applied were AMICAL, SF-36 and WOMAC for knee OA and AMICAL, SF-36 and Lequesne for coxarthritis. AMICAL was applied again after 72h to assess the consistency of the instrument (reattapplication).
Statistical AnalysisStatistical tests used were: for the agreement of the expert panel during transculturation, kappa index, and to evaluate the homogeneity of the samples during validation, the Mann–Whitney and χ.2 The clinimetric analysis for homogeneity of the AMICAL questionnaire was estimated with Cronbach α (α C), consistency estimated with CCI and correlation with other questionnaires was established using Spearman's rho. Statistical analysis was performed using SPSS software version 16.0, the chosen level of reliability was 95% with a power of 80. A P value less than .05 was considered significant.
ResultsIn transculturization, a pilot study was performed with 10 patients with OA and 10 subjects without it, homogeneous in age, with a median of 61 and 63 years, respectively (range 29, minimum 50 and maximum 79); the female gender predominated in both groups, 60% (6) and 70% (7), respectively. In the final analysis by the multidisciplinary panel and pilot testing, the following changes occurred in the items from the choice of options for Word 1 Word 2: Question 11: collective versus public; Question 15: morally versus depressed and Question 17: invalid versus disabled. The 1–10 scale of digital output of the questionnaire remained at the end and the panel concluded it had grammar and content equivalence.
In the validation to estimate the homogeneity, 100 patients were recruited for each type of OA, and for consistency 65 patients were recruited, for each type of arthritis (see Table 1).
Clinical and Demographic Characteristics of Patients With Knee OA and Coxarthrosis of the Study Sample, n knee OA=100, n Coxarthrosis=100.
| Variables | Knee OA | Coxarthrosis | ||
| Average | Standard deviation | Average | Standard deviation | |
| Age (years) | 56.34 | 13 | 60.1 | 9.2 |
| Percentage | Frequency | Percentage | Frequency | |
| Gender | ||||
| Female | 67 | 67 | 79.8 | 80 |
| Schooling | ||||
| Complete primary | 33 | 33 | 35.5 | 36 |
| Occupation | ||||
| Home | 38 | 38 | 52 | 52 |
| Laterality of osteoarthritis | ||||
| Bilateral | 72.7 | 644 | ||
| Right | 57.8 | 58 | ||
| Radiological stage | ||||
| II | 37 | 37 | ||
| III | 44.1 | 45 | ||
| Form of questionnaire filling | ||||
| AutoFill | 97 | 97 | 96 | 96 |
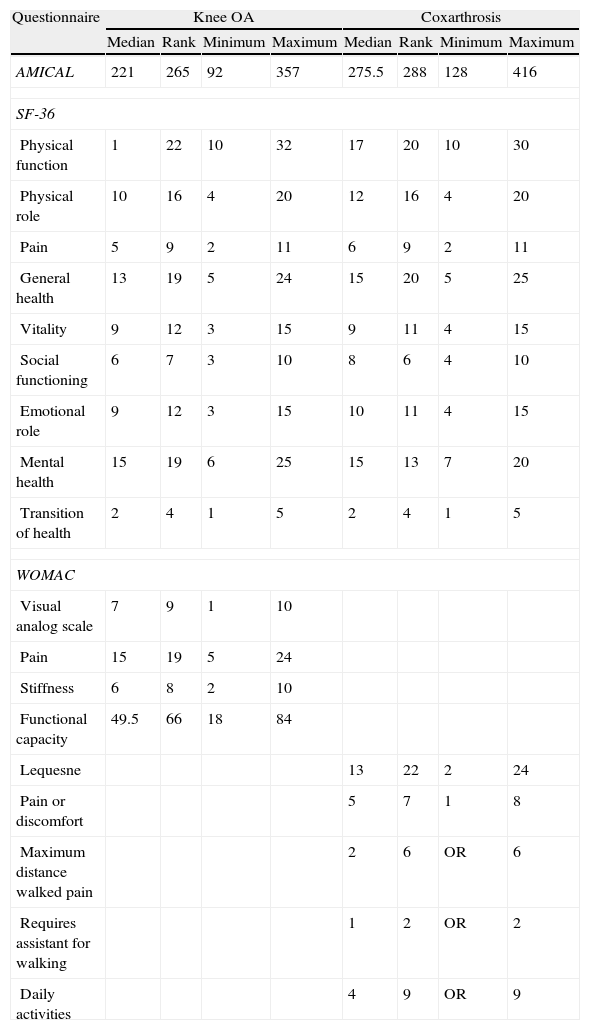
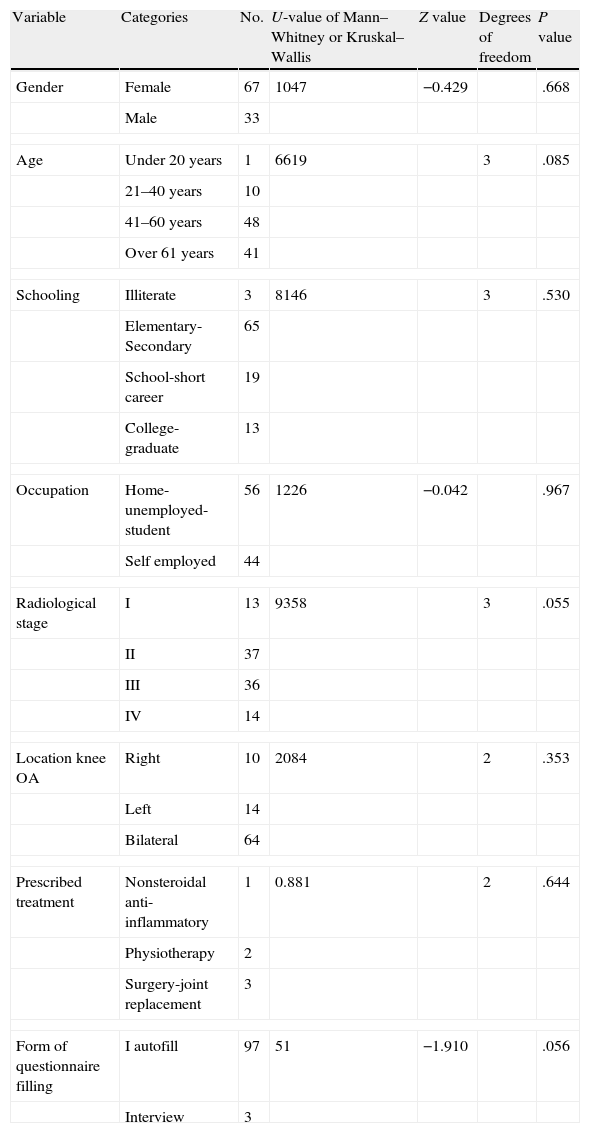
For the basic purposes of the study, the sum of scores or domains of the instruments was reversed so that higher scores meant better overall or specific QOL. Regarding the mode of application of the questionnaires, 97% were self-administered. The median total scores of the questionnaires is shown in Table 2. After the homogeneity analysis among the variables of the samples no significant differences in relation to the QOL (see Table 3) were found.
Characteristics of the Total Scores or by Domains of the Questionnaires Administered to Patients in the Sample, n knee OA=100 and n Coxarthrosis=100.
| Questionnaire | Knee OA | Coxarthrosis | ||||||
| Median | Rank | Minimum | Maximum | Median | Rank | Minimum | Maximum | |
| AMICAL | 221 | 265 | 92 | 357 | 275.5 | 288 | 128 | 416 |
| SF-36 | ||||||||
| Physical function | 1 | 22 | 10 | 32 | 17 | 20 | 10 | 30 |
| Physical role | 10 | 16 | 4 | 20 | 12 | 16 | 4 | 20 |
| Pain | 5 | 9 | 2 | 11 | 6 | 9 | 2 | 11 |
| General health | 13 | 19 | 5 | 24 | 15 | 20 | 5 | 25 |
| Vitality | 9 | 12 | 3 | 15 | 9 | 11 | 4 | 15 |
| Social functioning | 6 | 7 | 3 | 10 | 8 | 6 | 4 | 10 |
| Emotional role | 9 | 12 | 3 | 15 | 10 | 11 | 4 | 15 |
| Mental health | 15 | 19 | 6 | 25 | 15 | 13 | 7 | 20 |
| Transition of health | 2 | 4 | 1 | 5 | 2 | 4 | 1 | 5 |
| WOMAC | ||||||||
| Visual analog scale | 7 | 9 | 1 | 10 | ||||
| Pain | 15 | 19 | 5 | 24 | ||||
| Stiffness | 6 | 8 | 2 | 10 | ||||
| Functional capacity | 49.5 | 66 | 18 | 84 | ||||
| Lequesne | 13 | 22 | 2 | 24 | ||||
| Pain or discomfort | 5 | 7 | 1 | 8 | ||||
| Maximum distance walked pain | 2 | 6 | OR | 6 | ||||
| Requires assistant for walking | 1 | 2 | OR | 2 | ||||
| Daily activities | 4 | 9 | OR | 9 | ||||
Homogeneity of Patients With Knee Osteoarthritis Compared to the Clinical and Demographic Study Variables Relating to the Quality of Life With the AMICAL Questionnaire, n=100.
| Variable | Categories | No. | U-value of Mann–Whitney or Kruskal–Wallis | Z value | Degrees of freedom | P value |
| Gender | Female | 67 | 1047 | −0.429 | .668 | |
| Male | 33 | |||||
| Age | Under 20 years | 1 | 6619 | 3 | .085 | |
| 21–40 years | 10 | |||||
| 41–60 years | 48 | |||||
| Over 61 years | 41 | |||||
| Schooling | Illiterate | 3 | 8146 | 3 | .530 | |
| Elementary-Secondary | 65 | |||||
| School-short career | 19 | |||||
| College-graduate | 13 | |||||
| Occupation | Home-unemployed-student | 56 | 1226 | −0.042 | .967 | |
| Self employed | 44 | |||||
| Radiological stage | I | 13 | 9358 | 3 | .055 | |
| II | 37 | |||||
| III | 36 | |||||
| IV | 14 | |||||
| Location knee OA | Right | 10 | 2084 | 2 | .353 | |
| Left | 14 | |||||
| Bilateral | 64 | |||||
| Prescribed treatment | Nonsteroidal anti-inflammatory | 1 | 0.881 | 2 | .644 | |
| Physiotherapy | 2 | |||||
| Surgery-joint replacement | 3 | |||||
| Form of questionnaire filling | I autofill | 97 | 51 | −1.910 | .056 | |
| Interview | 3 | |||||
The α C in subjects with knee OA was 0.946 and in those with coxarthritis was 0.999, so it was significant for both profiles (P<0.05), which was maintained during analysis when removing one by one additional items as employment, family, public transport use and sexuality, as it applied to some patients and not others (α C 0.937–0.941, P<0.05).
ConsistencyReapplication after 72h was performed to assess the consistency, which was significant for both samples (0.979 CCI knee OA, 95%, from 0.961 to 0.991 and 0.998 coxarthrosis CCI, CI 0.997–0.999, P<0.05).
Correlation With Other InstrumentsAMICAL correlated with SF-36, WOMAC and Lequesne indexes, finding significant correlations for total score and most of the domains.
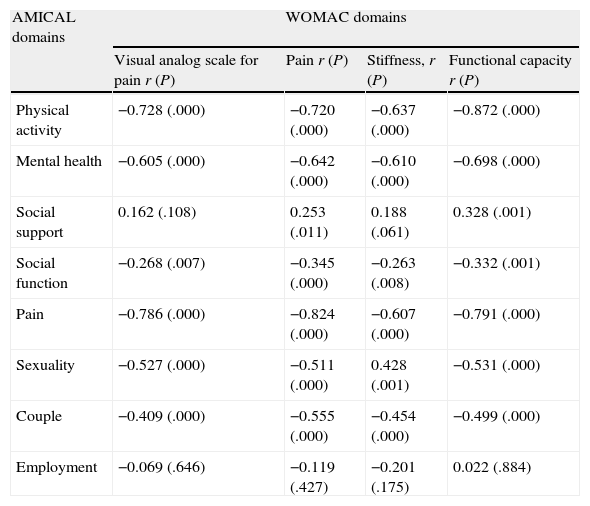
WOMAC Index in Knee OsteoarthritisAMICAL total score showed significant correlation (P<0.05) in their disaggregated domains for visual analog scale (VAS) (r 0.737), functional capacity (r −0.831), pain (r −0.742) and stiffness (r −0.649).
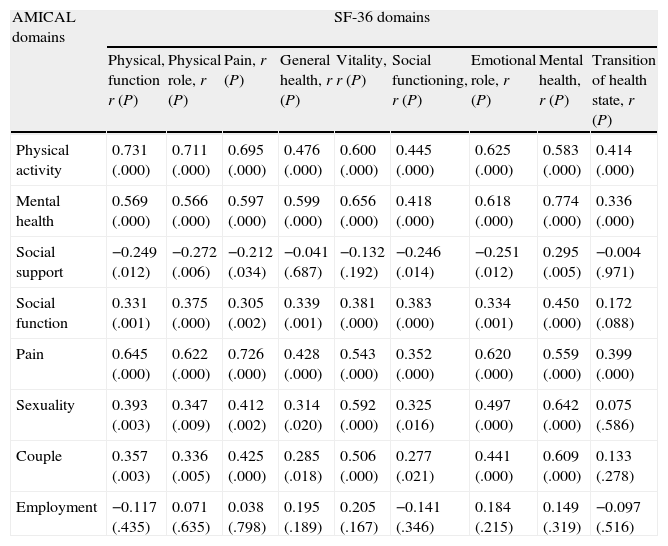
Knee Osteoarthritis Score by DomainsAMICAL correlations with WOMAC was high (r>0.6) and significant (P<0.05) for physical activity, mental health and pain (see Table 4). AMICAL correlations with SF-36 AMICAL were high (r>0.6) and significant (P<0.05): physical activity (with physical function, physical role, pain, vitality and emotional role), mental health (vitality, emotional role and mental health), pain (with physical function, physical role, pain and emotional role), sexuality (in mental health) and couples (with mental health) (see Table 5).
Correlations of the Domains of the WOMAC Questionnaire With the AMICAL Index in Patients With Knee Osteoarthritis, n=100.
| AMICAL domains | WOMAC domains | |||
| Visual analog scale for pain r (P) | Pain r (P) | Stiffness, r (P) | Functional capacity r (P) | |
| Physical activity | −0.728 (.000) | −0.720 (.000) | −0.637 (.000) | −0.872 (.000) |
| Mental health | −0.605 (.000) | −0.642 (.000) | −0.610 (.000) | −0.698 (.000) |
| Social support | 0.162 (.108) | 0.253 (.011) | 0.188 (.061) | 0.328 (.001) |
| Social function | −0.268 (.007) | −0.345 (.000) | −0.263 (.008) | −0.332 (.001) |
| Pain | −0.786 (.000) | −0.824 (.000) | −0.607 (.000) | −0.791 (.000) |
| Sexuality | −0.527 (.000) | −0.511 (.000) | 0.428 (.001) | −0.531 (.000) |
| Couple | −0.409 (.000) | −0.555 (.000) | −0.454 (.000) | −0.499 (.000) |
| Employment | −0.069 (.646) | −0.119 (.427) | −0.201 (.175) | 0.022 (.884) |
Correlations Between AMICAL Domains of SF-36 Questionnaire in Patients With Knee Osteoarthritis, n=100.
| AMICAL domains | SF-36 domains | ||||||||
| Physical, function r (P) | Physical role, r (P) | Pain, r (P) | General health, r (P) | Vitality, r (P) | Social functioning, r (P) | Emotional role, r (P) | Mental health, r (P) | Transition of health state, r (P) | |
| Physical activity | 0.731 (.000) | 0.711 (.000) | 0.695 (.000) | 0.476 (.000) | 0.600 (.000) | 0.445 (.000) | 0.625 (.000) | 0.583 (.000) | 0.414 (.000) |
| Mental health | 0.569 (.000) | 0.566 (.000) | 0.597 (.000) | 0.599 (.000) | 0.656 (.000) | 0.418 (.000) | 0.618 (.000) | 0.774 (.000) | 0.336 (.000) |
| Social support | −0.249 (.012) | −0.272 (.006) | −0.212 (.034) | −0.041 (.687) | −0.132 (.192) | −0.246 (.014) | −0.251 (.012) | 0.295 (.005) | −0.004 (.971) |
| Social function | 0.331 (.001) | 0.375 (.000) | 0.305 (.002) | 0.339 (.001) | 0.381 (.000) | 0.383 (.000) | 0.334 (.001) | 0.450 (.000) | 0.172 (.088) |
| Pain | 0.645 (.000) | 0.622 (.000) | 0.726 (.000) | 0.428 (.000) | 0.543 (.000) | 0.352 (.000) | 0.620 (.000) | 0.559 (.000) | 0.399 (.000) |
| Sexuality | 0.393 (.003) | 0.347 (.009) | 0.412 (.002) | 0.314 (.020) | 0.592 (.000) | 0.325 (.016) | 0.497 (.000) | 0.642 (.000) | 0.075 (.586) |
| Couple | 0.357 (.003) | 0.336 (.005) | 0.425 (.000) | 0.285 (.018) | 0.506 (.000) | 0.277 (.021) | 0.441 (.000) | 0.609 (.000) | 0.133 (.278) |
| Employment | −0.117 (.435) | 0.071 (.635) | 0.038 (.798) | 0.195 (.189) | 0.205 (.167) | −0.141 (.346) | 0.184 (.215) | 0.149 (.319) | −0.097 (.516) |
The total score of AMICAL showed low (r −0.383) but significant correlation (P<0.05).
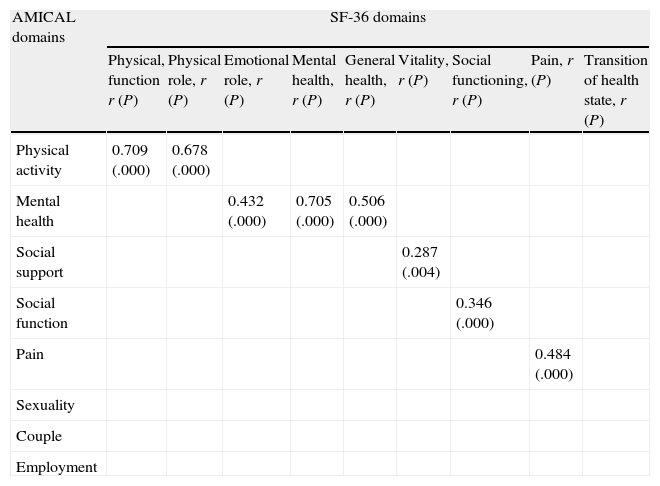
Coxarthrosis Score by DomainAMICAL correlations with SF-36 were high (r>0.6) and significant (P<0.000) for: physical activity with physical functioning (r 0.709) and physical role (r 0.678) and mental health with mental health (r 0.705) and to a lesser degree with general health (r 0.506) and emotional role (r 0.432). In other domains, the correlations were low but significant: pain with pain (r 0.484), social function with social functioning (r 0.346) and social support with vitality (r 0.287) (see Table 6).
Significant Correlations of AMICAL Domains of SF-36 Questionnaire in Patients with Coxarthritis, n=100.
| AMICAL domains | SF-36 domains | ||||||||
| Physical, function r (P) | Physical role, r (P) | Emotional role, r (P) | Mental health, r (P) | General health, r (P) | Vitality, r (P) | Social functioning, r (P) | Pain, r (P) | Transition of health state, r (P) | |
| Physical activity | 0.709 (.000) | 0.678 (.000) | |||||||
| Mental health | 0.432 (.000) | 0.705 (.000) | 0.506 (.000) | ||||||
| Social support | 0.287 (.004) | ||||||||
| Social function | 0.346 (.000) | ||||||||
| Pain | 0.484 (.000) | ||||||||
| Sexuality | |||||||||
| Couple | |||||||||
| Employment | |||||||||
Throughout the study, it was shown that AMICAL is simple, reproducible and valid compared to other general and specific instruments for lower limb OA, and a good correlation was found, except for the Lequesne index for osteoarthritis. In patients with knee OA, the specific QOL determined by physical activity, mental health and pain, found a significant association in the amount of pain reported by the patient, functional ability and manifested in WOMAC by stiffness. As for the SF-36, higher associations with at least one of the domains, except for the AMICAL domain of social support, social function and employment was seen. In osteoarthritis, the specific QOL was moderately associated with SF-36, except in the case of the latter for social support, social function, pain, sexuality, family and employment. With the Lequesne index, the association was low but significant, which can be explained by the domains assessed, as it is directed specifically to the degree of disability of the patient according to the severity of the OA.22
All instruments evaluated in the study focused on the pain and how its affects the whole activities of the individual regarding QOL10; however, AMICAL evaluates certain exclusive domains (social support, clinical behavior during sleep, planning ahead, adverse effects of medication, perceived emotional aspects with physical dysfunction that causes them to feel observed by another person, using public transportation, difficulty starting off after repeated positions and aspects such as dating and sexuality) that are not scanned in SF-36.17,20 Although WOMAC assessed stiffness, it is usually associated with pain, AMICAL also includes the emotional aspect and the perception of it, like other instruments, such as EuroQol regarding physical health17,21 but the latter, for example, has no domains included for couples, sexuality or transport.17,19 As Lequesne, within this study found a significant but low correlation, suggesting we consider the application of the instrument separately.17,22
During the analysis of the psychometric properties, a demographic analogy and clinical profile of patients were seen in relation to the original validation in French: Average age was 56, 34+13 years versus 66 years, female gender 60n1% versus 59%, same primary schooling, a similar percentage of affected joint in coxarthrosis and knee OA: 50%/50% versus 56%/44%, the time of completion of the questionnaire was consistent in a range of 15–20min and the time was different for reapplication 3 days after the initial application for AMICAL in Spanish versus 10 days for the French version, although the minimum time to avoid recall bias is usually 3 days. A high degree of homogeneity was seen in both validations (from 0.946 to 0.999 in Spanish versus 0.910 to 0.960 in French) and only for social support and social functioning, this was lower (0.73–0.81). Consistency in the reapplication was high for both versions (from .961 to .999 versus .53 to .91). The correlation with other instruments was significant for the total score and most of the domains, in the same way as that of the French version, for example in the SF-36 physical functioning, physical activity and physical role (r 0.50–0.63) mental health or mental health and vitality (r 0.66–0.75), showed moderate or low correlations, such as pain in the WOMACs VAS domain (r 0.42).17
The study is comparable with its French original validation, in which patients with OA were evaluated postoperative, because the version of the AMICAL questionnaire validated in this study has also been used in monitoring the change in the QoL of patients with knee OA after application of 2 types of rehabilitation intervention in independent samples through a controlled clinical trial.23 Furthermore, a limitation of the original study in France was, as the authors state, that “the instrument was evaluated only in France but the relevance and psychometric properties in other countries and cultures remains unknown.” This study is of great importance as it validates an instrument in a language spoken natively worldwide17 considering the Spanish-speaking population one with a rapid growth rate, s with increased susceptibility of migration, such as in Latin America and Europe.
Therefore, the AMICAL questionnaire retains adequate clinimetric properties in relation to the original version and is feasible to apply in our setting. This occurs in relation to the migratory movement of the growing Spanish-speaking people around the world, the birth and residence of the largest population with that feature in at least 19 countries in different continents of the world, with Spanish positioned between the second and fourth language most spoken in countries with a different native language. It is essential then to have such a tool, similar to the original validation, validated instruments available with which to identify or monitor the QOL for research, implementation and evaluation of therapeutic strategies or applied, after taking account the cultural adaptation necessary for each region or Spanish-speaking country.11,13,15–22 The use of the questionnaire in daily practice is recommended, as well as for epidemiological studies and even clinical trials, which could assess their external validity.
Ethical ResponsibilitiesProtection of people and animalsThe authors declare that no experiments have been performed on humans or animals.
Data PrivacyThe authors state that patient data does nor appear in this article.
Right to privacy and informed consentThe authors state that patient data does not appear in this article.
Conflict of InterestThe authors have no conflicts of interest.
CONACYT Grant Funding number 207227 and IMSS grant. Acknowledgements: Health Education Coordination and Outpatient Area, Rehabilitation Unit Siglo XXI and Orthopedics Department, General Regional Hospital 1, Mexican Social Security Institute, Mexico City, Mexico.
The following are the supplementary data to this article:
Please cite this article as: Espinosa-Cuervo G, Guillermin F, Rat A-C, Duarte-Salazar C, Alemán-Hernández S-I, Vergara-Álvarez Y, et al. Transculturización y validación al español del Cuestionario específico de artrosis de miembros inferiores y calidad de vida AMICAL: Arthrose des Membres Inférieurs et Qualité de vie AMIQUAL. Reumatol Clin. 2014;10:241–247.


