





Transient osteoporosis of the hip (TOH) can occur in the context of pregnancy. In this case, it often develops in the last trimester and, to a lesser extent, before or after labor. It is usually unilateral and most likely to occur on the left side.1–3 Because it is uncommon, we present the case of bilateral TOH, with greater involvement of the right side, during the fifth month of pregnancy.
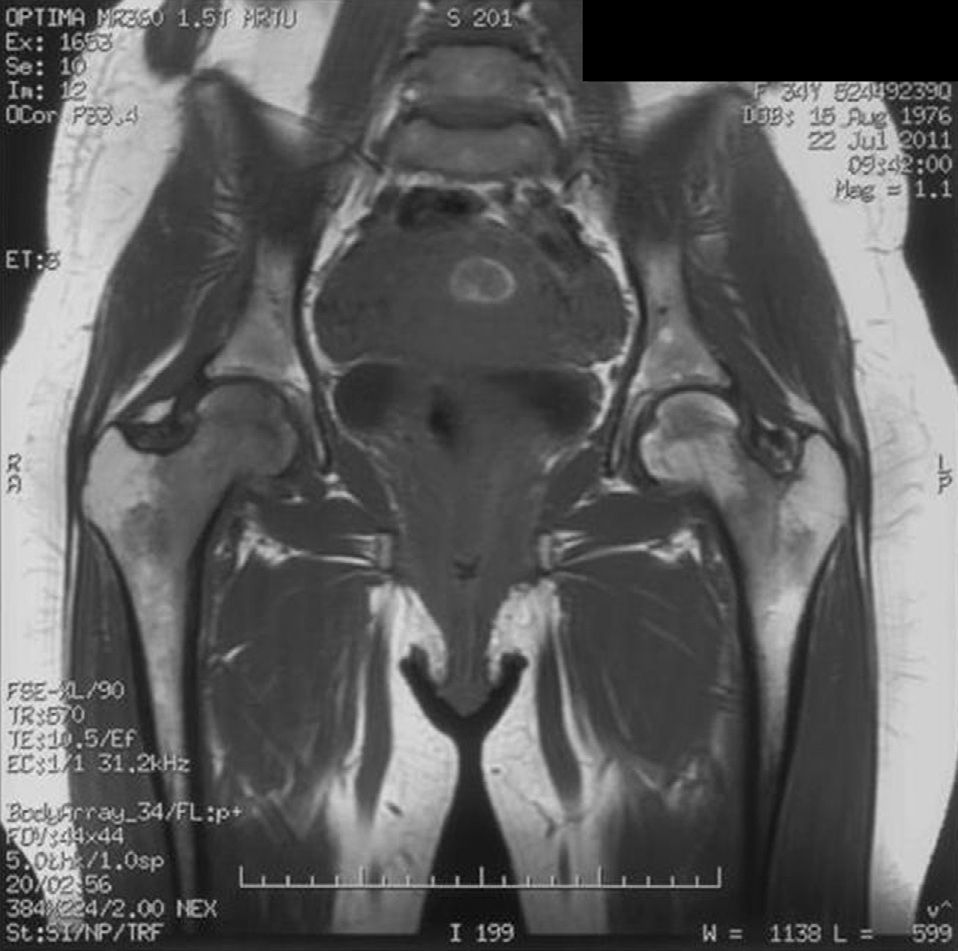
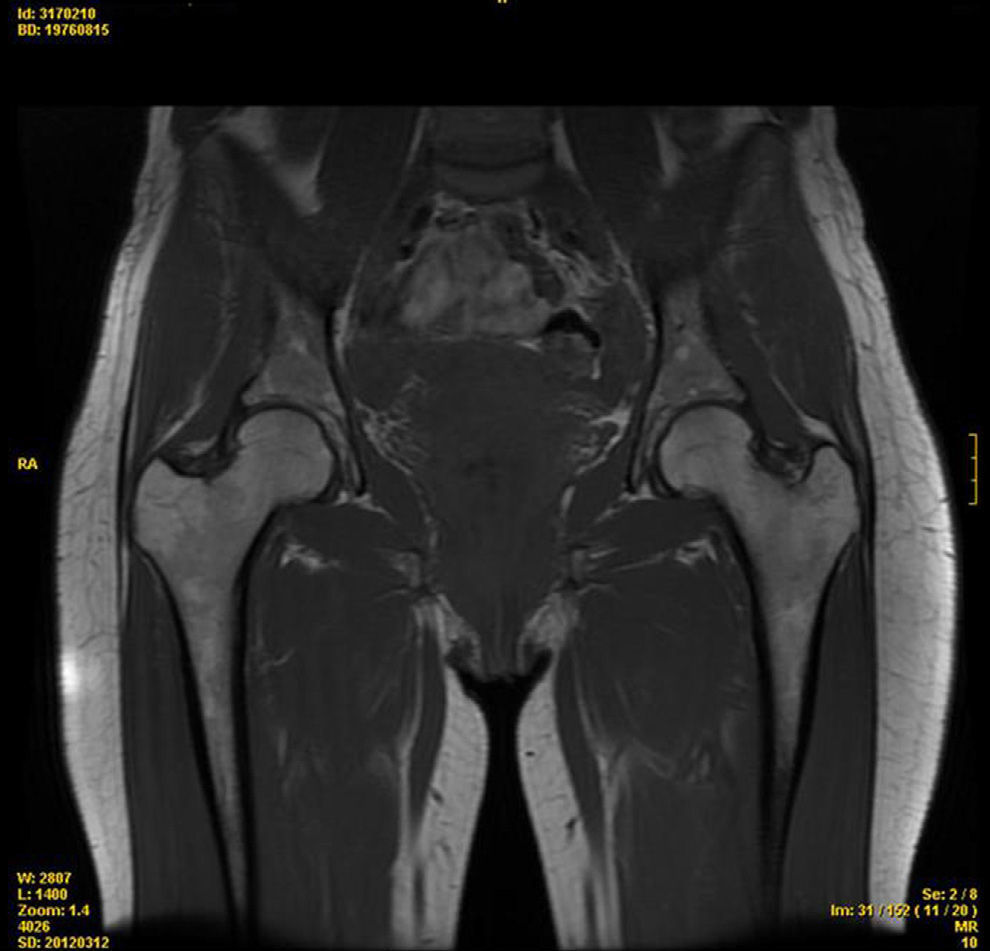
The patient was a 34-year-old woman undergoing her first pregnancy with a history of idiopathic left hip TO, which occurred six years earlier. During the fifth month of pregnancy and with no other known trigger, she began to have pain in the right buttock which was attributed to a pyramidal bone syndrome. Afterwards, the pain was located on the outside of the right hip and was classified as a probable trochanteritis. In the absence of improvement, she was referred to rheumatology during the seventh month of pregnancy. She complained of pain on the lateral side of both hips, more markedly on the right, accompanied by significant functional impairment. This pain was compounded by weight burden and gait, forcing her to use crutches. The examination revealed pain and limitation in abduction and external rotation of the right hip, without alterations in other areas of the musculoskeletal system. Otherwise, laboratory data did not see an increase in acute phase reactants, with negative rheumatoid factor, citrullinated peptide antibodies and HLAB27. There was no radiological or scintigraphic study performed due to the pregnancy. Suspecting a TOH, she was treated with paracetamol, physiotherapy and unloading of the joint. During the postpartum period, we performed an X-ray which showed no abnormalities, and an MRI in which “intraspongy cephalic and intertrochanteric right and left marrow edema, with no signs of osteonecrosis or sacroiliitis, all of this indicating a bilateral TOH” (Fig. 1). After the birth, she had progressive improvement and the symptoms disappeared after 2 months. In a second imaging control, at eighth months postpartum, there was a restoration of normalcy in the MR images (Fig. 2).
Prevalence of TOH due to pregnancy is difficult to assess. It usually occurs in the last third of pregnancy and to a lesser extent, before or postpartum. Its pathogenesis is unclear and, therefore, involves several factors: microtrauma, trabecular microfractures by decreased bone mass during pregnancy, circulatory changes characteristic of pregnancy and compression of the obturator or pelvic sympathetic nerve by the gravid uterus. Clinically, it usually presents with groin pain or pain adjacent to the hip, of a mechanical rhythm, accompanied by functional impairment. The preference for the left hip is allegedly due to cephalic presentation of the fetus, which could lead to repeated microtrauma in that area. Bilateral involvement is exceptional. Similarly, migratory forms have been described affecting the knee, ankle or foot. Laboratory changes only relate to those seen during pregnancy. Initially, X-rays are normal and later (1–2 months), a homogeneous demineralization, that does not affect the joint line may be seen. Early on scintigraphy shows increased uptake of isotope in the acetabulum and femur. MRI is essential for diagnosis, showing edema in the affected area and ruling out osteonecrosis, as in the present case. It is convenient to make a differential diagnosis with other hip problems (osteonecrosis, inflammatory rheumatic disease, infectious disease, metabolic disease, synovial disease, neoplasia, osteomalacia and trauma) or surrounding area disorders (lumbar, sacroiliac, symphysis pubis, uro-genital and digestive). Treatment is based on the joint unloading, analgesia and physical therapy. It usually has a favorable outcome and recovery without sequelae in variable periods of time (2 months to 1 year). However, some cases leading to osteonecrosis or femoral neck fracture have been described.1–8
In sum, we consider it necessary to rule out the presence of primary TOH when there is groin or hip pain in a pregnant woman. Similarly, early diagnosis is important using scintigraphy and MRI when circumstances permit. In addition, early treatment is essential for a quick recovery. Finally, it is important to monitor a possible progression toward osteonecrosis or fracture of the femoral neck.
Please, cite this article as: Bruscas Izu C, San Juan de la Parra S. Osteoporosis transitoria de ambas caderas en el embarazo. Reumatol Clin. 2014;10:58–59.


