






Evidence evaluating the association between pre-frailty and frailty, and risk of adverse health outcomes in patients with Behçet's syndrome (BS) is limited in the literature. The aim of this study was to characterize the prevalence of frailty and associated factors in a single-centre cohort of patients with BS.
MethodsBased on the International Study Group's criteria, this was a monocentric cross-sectional study of BS patients. The Fried frailty criteria were used to define frailty. The Turkish version of the Behçet's Disease Current Activity Form was used to measure the disease activity of BS. Damage index was assessed with the Behçet's Syndrome Overall Damage Index.
ResultsForty-four patients were enrolled. According to Fried frailty criteria, patients were classified as 13.6% frail, 59% pre-frail, and 27.2% robust, respectively. Compared to pre-frail and robust patients, frail patients had higher levels of inflammatory markers at the time of diagnosis. CRP levels at time of diagnosis and at the last visit were higher in the frail group than in the pre-frail and robust groups (p=0.039 and p=0.023, respectively). When active drugs for BS were evaluated, systemic glucocorticoid (50%, p=0.030) and cyclophosphamide (33.3%, p=0.006) treatments were higher in the frail group.
ConclusionsFrailty and pre-frailty are commonly detected even in younger patients with BS. Inflammation can be described as potential determinants of frailty status.
La evidencia que evalúa la asociación entre prefragilidad y fragilidad, y el riesgo de resultados adversos para la salud en los pacientes con síndrome de Behçet (SB) es limitada en la literatura. El objetivo de este estudio fue caracterizar la prevalencia de fragilidad y los factores asociados en una cohorte de pacientes con SB.
MétodosBasado en los criterios del Grupo Internacional de Estudio, este fue un estudio monocéntrico transversal de pacientes con SB. Se utilizaron los criterios de fragilidad de Fried para definir la fragilidad. Se utilizó la versión turca del Behçet's Disease Current Activity Form para medir la actividad de la enfermedad. El índice de daño se evaluó con el Índice de Daño Global del Síndrome de Behçet.
ResultadosSe incluyeron 44 pacientes. Según los criterios de fragilidad de Fried, los pacientes fueron clasificados como 13,6% frágiles, 59% prefrágiles y 27,2% robustos, respectivamente. En comparación con los pacientes prefrágiles y robustos, los pacientes frágiles tenían niveles más altos de marcadores inflamatorios en el momento del diagnóstico. Los niveles de PCR en el momento del diagnóstico y en la última visita fueron más altos en el grupo frágil que en los grupos prefrágil y robusto (p=0,039 y p=0,023, respectivamente). Cuando se evaluaron los fármacos activos para el SB, los tratamientos sistémicos con glucocorticoides (50%, p=0,030) y ciclofosfamida (33,3%, p=0,006) fueron mayores en el grupo frágil.
ConclusionesLa fragilidad y la prefragilidad se detectan comúnmente incluso en pacientes jóvenes con SB. La inflamación puede ser descrita como un potencial determinante del estado de fragilidad.
Frailty is a syndrome marked by a reduction in the physiologic reserve and function of multiple systems, making a person more susceptible to stressors and poor health outcomes, such as hospitalization, falls, disability, and death.1 Individuals with chronic conditions have been found to have a higher prevalence of frailty, and research has shown that frailty is an independent predictor of unfavourable outcomes.2,3 In addition to placing a serious burden on healthcare systems, frailty may increase mortality and morbidity.4 Chronic low-grade elevation of inflammatory markers, such as interleukin-6 (IL-6) and, C-reactive protein (CRP) has been linked to frailty; this condition is known as “inflammageing”.5,6 Moreover, IL-6 and other markers have demonstrated a higher correlation with mortality and functional dependence as well as frailty than age.7,8
Behçet syndrome (BS) is a unique chronic systemic inflammatory disease of unknown aetiology. It is defined by recurrent mucocutaneous lesions and major organ involvements such as ocular, neurologic, vascular, and gastrointestinal manifestations.9 Because BS affects venous and arterial vessels of all sizes, it was classified as a variable-vessel vasculitis by the revised Chapel Hill Consensus Conference.10 The second and third decades of life are often when BS first appears, and it progresses through a remitting-relapsing course with a decline in disease activity as people age.9 BS is also characterized by increased proinflammatory markers, such as CRP, IL-6 and tumour necrosis factor alpha (TNF-α). Ocular, major vascular, central nervous system, and gastrointestinal involvement potentially present life-long disability, including blindness, or can even be lethal.11 Corticosteroids and immunosuppressive drugs are used in the treatment. Major organ manifestations, systemic inflammation, use of glucocorticoids and immunosuppressive drugs may contribute to frailty in this patient group.
Pre-frailty and frailty are conditions,4 that can be prevented and have irreversible effects, particularly if detected early on,12 therefore, it may be required to evaluate the parts of frailty syndrome in clinical practice to enhance patients’ global health status. Pre-frailty is a condition that manifests earlier on the frailty spectrum and is linked to the later condition's development. Therefore, pre-frailty might be a better candidate for screening and implementation in order to facilitate early interventions.13,14 Frailty can occur in any age group and is most commonly observed in older adults with chronic diseases, such as rheumatic disorders.4 Many rheumatic diseases have been reported to exhibit frailty.15
Patients with BS are anticipated to be at higher risk of frailty due to multiorgan manifestations, systemic inflammation, exposure to glucocorticoid and immunosuppressive therapies, however, the prevalence of frailty and factors associated with frailty have not been identified in BS patients yet. The objective of this study was to describe the prevalence of frailty in patients with BS, and describe its association with demographics and clinical characteristics.
Materials and methodsStudy designThis study was carried out in compliance with the ethical guidelines established by the 1964 Declaration of Helsinki and its subsequent amendments as a single-centre cross-sectional cohort study at the Rheumatology Clinic of Bilkent City Hospital, with approval from the institutional ethics committee (IRB no. E2-22-2454).
The research was carried out in 2022 between August and December. A thorough clinical and physical examination was used to evaluate each patient with BS after they were included.
PatientsPatient group included adult BS patients who met criteria of International Study Group (ISG).16 Exclusion criteria included end-stage chronic renal failure, stroke, severe liver failure, severe chronic obstructive pulmonary disease, cardiopulmonary and muscle involvement of BS, pulmonary hypertension, Hughes-Stovin Syndrome, chronic infections, concurrent malignancy, cognitive impairment, and patients under the age of 18. Written informed consent was signed by each patient.
Data collectionClinical and demographic information, including age, gender, body mass index (BMI), length of illness, and employment status, comorbidities, ongoing medications, disease activity status, clinical manifestations, data on organs damage, and smoking habits were collected for each patient from our hospital records. Initial and current glucocorticoid dose and use of non-steroidal agents, if available, were obtained from review of hospital records during eligibility screening. At the time of the study visit, the available dose of glucocorticoids was verified. ESR and CRP, both at the time of diagnosis and most recent measurements were obtained from hospital records. Information on glucocorticoid-related adverse events reported by individuals was also collected. Disease activity was measured using those provided by treating physicians. The Turkish version of the Behçet's Disease Current Activity Form (BDCAF) was used to measure the disease activity of BS.17 The BDCAF assesses the presence of symptoms in 12 clinical categories during the four weeks preceding the assessment day. Oral and genital ulcers, arthralgia, arthritis, skin pustules, erythema nodosum, vomiting or nausea or abdominal pain, diarrhoea or hematochezia, headache, and symptoms pertaining to the nervous system, major vessels, and eyes are among the clinically observed symptoms. The Behçet's Syndrome Overall Damage Index (BODI) was used to measure disease damage.18 The BODI scale was created especially to help BD patients identify and quantify organ damage. The 34 items that make up the BODI are divided into nine organ/system areas: vascular, cardiovascular, neuropsychiatric, gastrointestinal, reproductive, mucocutaneous, musculoskeletal, and other. The overall score goes from 0 to 46, with 1 point assigned to each item and subitem. Pathologies lasting longer than six months were considered to cause organ damage.
Definition of the frailty phenotypeBased on the five criteria put forth by Fried et al.,19 the participants’ frailty status was assessed. The five criteria that make up the Fried frailty definition are as follows: (1) low BMI or weight loss (≤18.5kg/m2 or self-report as having lost at least 10 pounds in the previous year); (2) exhaustion [measured by two items from the Center for Epidemiological Studies Depression scale (CESD)]; (3) inactivity/low energy consumption (defined as energy expenditure of less than 383kcal/week in men and 270kcal/week in women); (4) slow 4-m gait speed (men: ≥7s for height ≤1.73m and ≥6s for height >1.73m; women: ≥7s for height ≤1.59m and ≥6s for height >1.59m); and (5) low grip strength (based on following criteria; men: ≤29 for BMI <24, ≤30 for BMI 24.1–28, and ≤32 for BMI >28; female: ≤17 for BMI <2 3, ≤17.3 for BMI 23.1–26, ≤18 for BMI 26.1–29, and ≤21 BMI >29.). Patients who meet three or more criteria are classified as frail; those who meet just one or two criteria are classified as pre-frail; and those who meet no criteria are classified as robust.
Statistical analysisThe Statistical Package for the Social Sciences (SPSS) version 22 was used for statistical analysis (IBM Corp., Armonk, NY, USA). The normality of variables was examined using both analytical (Kolmogorov–Smirnov test) and visual (histogram and probability graphics) methods. Depending on the normality of the data, descriptive statistics are displayed as mean±standard deviation or as median and interquartile range (IQR). Categorical variables were represented by numbers and percentages. Different tests were used to compare continuous variables for normality: the Student-t test or the Mann–Whitney U test. To evaluate categorical variables, the Fisher's final test and the χ2 test were utilized. Statistical significance was accepted when p values <0.05.
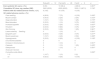
ResultsForty-four subjects who were enrolled all completed the study visit. The median age was 42 (IQR 13.5) years, 22 (50%) patients were women, and median disease duration 108.0 (IQR 112.0) months (Table 1).
Demographics and clinical characteristics of BS patients and comparisons according to frailty status.
| All patientsN=44 | RobustN=12 | Pre-frailN=26 | FrailN=6 | p | |
|---|---|---|---|---|---|
| Age, years, median (IQR) | 42.0 (13.5) | 37.5 (17.5) | 42.0 (14.0) | 43.5 (26.5) | 0.160a |
| Gender, female,n(%) | 22 (50) | 6 (50) | 12 (46.2) | 4 (66.7) | 0.380a |
| BMI, kg/m2, median (IQR) | 25.0 (5.8) | 23.5 (10.5) | 27.0 (4.0) | 28.0 (15.8) | 0.249a |
| Ever smokers,n(%) | 15 (34.1) | 5 (41.7) | 8 (30.7) | 2 (33.3) | 0.735a |
| Regular exercise,n(%) | 4 (9.1) | 1 (8.3) | 2 (7.7) | 1 (16.7) | 0.487a |
| Comorbidities,n(%) | |||||
| Hypertension | 6 (13.6) | 0 | 4 (15.3) | 2 (33.3) | 0.130a |
| Diyabetes mellitus | 5 (11.4) | 1 (8.3) | 2 (7.7) | 2 (33.3) | 0.068a |
| Coroner artery disease | 1 (2.3) | 0 | 1 (3.8) | 0 | 0.688a |
| Chronic kidney disease | 2 (4.5) | 0 | 1 (3.8) | 1 (16.7) | 0.125a |
| COPD/asthma | 2 (4.5) | 0 | 1 (3.8) | 1 (16.7) | 0.125a |
| Depression | 1 (2.3) | 0 | 0 | 1 (16.7) | 0.011a |
| BS manifestations,n(%) | |||||
| Oral aphthae | 44 (100) | 12 (100) | 26 (100) | 6 (100) | 1 |
| Genital aphthae | 33 (75) | 7 (58.3) | 22 (84.6) | 4 (66.7) | 0.612a |
| Papulopustular eruption | 27 (61.4) | 0 | 22 (84.6) | 5 (83.3) | 0.660a |
| Erythema nodosum | 13 (29.5) | 7 (58.3) | 5 (19.2) | 1 (16.7) | 0.457a |
| Arthralgia | 19 (43.2) | 4 (33.3) | 12 (46.2) | 3 (50) | 0.717a |
| Arthritis | 12 (27.2) | 4 (33.3) | 7 (26.9) | 1 (16.7) | 0.530a |
| Sacroiliitis | 2 (4.5) | 0 | 1 (3.8) | 1 (16.7) | |
| Uveitis | 10 (22.7) | 6 (50) | 4 (15.4) | 0 | 0.153a |
| Neurological involvement | 8 (18.1) | 2 (16.7) | 4 (15.4) | 2 (33.3) | 0.300a |
| Gastrointestinal involvement | 2 (4.5) | 0 | 0 | 2 (33.3) | 0.010a |
| Vascular involvement | 14 (31.8) | 2 (16.7) | 8 (30.8) | 4 (66.7) | |
| Thrombosis | 10 | 2 | 6 | 2 | 0.505a |
| Aneurysm | 0 | 0 | 0 | 0 | |
| Age of symptom onset, years, median (IQR) | 27.0 (13.5) | 21 (19.8) | 25 (10) | 35.5 (10.8) | 0.024a |
| Age of diagnosis, years, median (IQR) | 32.0 (15.5) | 28 (19.5) | 29 (16) | 37.0 (21.5) | 0.045a |
| Disease duration, months, median (IQR) | 108.0 (112.0) | 114 (101) | 96 (134) | 102 (92.8) | 0.986a |
| CRP at diagnosis (mg/l), median (IQR) | 10 (5–37) | 16.5 (10–40) | 6 (4–20) | 32 (20–52) | 0.039 |
| ESR at diagnosis (mm/h), median (IQR) | 19.5 (11.5–35) | 29 (20.5–41) | 15 (8–25) | 26.5 (14–40) | 0.061 |
| CRP (mg/l), median (IQR) | 2.5 (1–5) | 3.5 (1–5.5) | 2 (1–5) | 15 (5–21) | 0.023 |
| ESR (mm/h), median (IQR) | 6 (5–14) | 8 (5–16) | 5 (5–12) | 16 (6–35) | 0.014 |
| BDCAF score, median (IQR) | 1.0 (1.0) | 0.5 (1) | 1.0 (1.0) | 1 (1.8) | 0.329a |
| BODI score, median (IQR) | 1.0 (1.0) | 0.5 (1) | 1.0 (1.0) | 1 (2.0) | 0.438a |
| Active medications for BS,n(%) | |||||
| Systemic glucocorticoids | 8 (18.1) | 3 (25) | 2 (7.7) | 3 (50.0) | 0.030a |
| Colchicine | 35 (79.5) | 10 (83.3) | 21 (80.8) | 4 (66.7) | 0.400a |
| Sulfasalazine | 1 (2.3) | 0 | 1 (3.8) | 0 | 0.688a |
| Azathiopurine | 7 (15.9) | 4 (33.3) | 3 (11.5) | 0 | 0.252a |
| Cyclophosphamide | 3 (6.8) | 0 | 1 (3.8) | 2 (33.3) | 0.006a |
| Infliximab | 2 (4.5) | 0 | 2 (7.7) | 0 | 0.565a |
| Adalimumab | 2 (4.5) | 1 (8.3) | 1 (3.8) | 0 | 0.565a |
| Depo-penicillin | 2 (4.5) | 1 (8.3) | 1 (3.8) | 0 | 0.565a |
| Warfarin | 3 (6.8) | 0 | 2 (7.7) | 1 (16.7) | 0.303a |
Abbreviations: BS: Behçet syndrome; COPD: chronic obstructive pulmonary disease; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; IQR: interquartile range; max: maximum; min: minimum.
Based on Fried frailty criteria, 6 (13.6%), 26 (59%) and 12 (27.2%) patients were classified as frail, pre-frail and robust, respectively (Table 1 and Fig. 1). Frail patients were older, with a median age of 43.5 years (IQR 26.5), and more commonly were female (66.7%). With a median age of 42 years (IQR 14), pre-frail patients were older than robust patients and more frequently male (53.8%).

Pre-frail and frail patients had more burden of comorbidities than robust patients. Among BS manifestations, gastrointestinal system findings were more common in the frail group (p=0.010), but other findings were similar in all groups (p>0.05). Age of symptom onset (IQR 35.5, p=0.024) and age at diagnosis (IQR 37.5, p=0.045) were higher in the frail group, and duration of disease was similar in all groups (p=0.986).
CRP levels at time of diagnosis differed among robust, pre-frail, and frail patients [median 16.5 (IQR 10.0, 40.0) vs 6 (4.0, 20.0) vs 32.0 (IQR 22.0, 50.0)mg/l, respectively], and higher in frail group, however, at the time of diagnosis, there was no discernible difference in ESR. No difference was observed for ESR at the time of the study visit, but CRP values were higher in the frail group than in the pre-frail and normal groups [median 15 (IQR 5.0, 21.0) vs 3.5 (1.0, 5.5) vs 2.0 (IQR 1.0, 5.0)mg/l, respectively)].
Systemic glucocorticoids (50%, p=0.030) and cyclophosphamide (33.3%, p=0.006) treatments were higher in the frail group when active drugs were evaluated for Behçet's syndrome. Although disease activity score BDCAF (p=0.329) and damage index BODI (p=0.438) score were higher in the frail group, they were not statistically significant (Table 1).
Frailty componentsWhen the frequency of subfield positivity was evaluated, the most common criterion met by the patients was exhaustion (33/44, 75%), followed by weakness (18/44, 40.9%). Slowness was the least encountered criterion and was met by only one (2.3%) patient (Table 2).
Total and subdomain frailty scores in patients.
| All patientsN=44 | RobustN=12 | Pre-frailN=26 | FrailN=6 | |
|---|---|---|---|---|
| Total frailty score, median (IQR) | 1 (2) | 0 | 1 (1) | 3 |
| Frequency of subdomain positivity, n (%) | ||||
| Exhaustion | 33 (75) | 4 (33.3) | 23 (88.5) | 6 (100) |
| Weakness | 18 (40.9) | 1 (8.3) | 11 (42.3) | 6 (100) |
| Inactivity | 4 (9.1) | 0 | 0 | 4 (66.7) |
| Slowness | 1 (2.3) | 0 | 0 | 1 (16.7) |
| Weight loss | 3 (6.8) | 0 | 2 (7.7) | 1 (16.7) |
Systemic glucocorticoid (GC) use was higher in the frail group (4/6, 66.6%). All patients using GCs noticed experiencing at least one GC-related adverse event, and most patients reported experiencing three or more. The reported frequency of individual GC-related adverse events and the cumulative frequency of such events among patients by frailty classification did not differ statistically significantly. (Table 3).
Relations between systemic glucocorticoid use and frailty status among 20 ever systemic glucocorticoid users.
| RobustN=12 | Pre-frailN=26 | FrailN=6 | p | |
|---|---|---|---|---|
| Ever systemic GC users, n (%) | 6 (50) | 10 (38.4) | 4 (66.6) | 0.261a |
| Cumulative GC dose, mg, median (IQR) | 3900 (6530) | 6000 (6025) | 5500 (11,687.5) | 0.740a |
| Patients with GC-related adverse events, n (%) | 6 (100) | 10 (100) | 4 (100) | |
| GC-related adverse events, n (%) | ||||
| Face swelling | 4 (66.6) | 7 (70) | 4 (100) | 0.430a |
| Muscle cramps | 3 (50.0) | 2 (20) | 2 (50) | 0.372a |
| Sleep disorders | 1 (16.7) | 1 (10) | 1 (25) | 0.770a |
| Mood disorders | 2 (33.3) | 1 (10) | 3 (75) | 0.055a |
| Increased appetite | 2 (33.3) | 5 (50) | 3 (75) | 0.637a |
| Hirsutism | 2 (33.3) | 8 (80) | 3 (75) | 0.837a |
| Skin thinning | 2 (33.3) | 3 (30) | 1 (25) | 0.961a |
| Lower extremitySwelling | 0 | 1 (10) | 0 | 0.591a |
| Epigastric pain | 2 (33.3) | 3 (30) | 3 (75) | 0.277a |
| Muscle weakness | 1 (16.7) | 4 (40) | 2 (50) | 0.499a |
| Hyperglycemia | 2 (33.3) | 6 (60) | 4 (100) | 0.108a |
| Uncontrolled diabetes | 0 | 0 | 0 | |
| Increase in blood pressure | 0 | 1 (10) | 0 | 0.501a |
| Cataracts | 0 | 1 (10) | 1 (25) | 0.435a |
| Osteoporosis | 0 | 1 (10) | 0 | 0.591a |
| Avascular necrosis | 0 | 0 | 0 | |
| Cumulative side effects | 0.690a | |||
| 1–2 | 1 (16.7) | 1 (10) | 0 (0) | |
| ≥3 | 5 (83.3) | 9 (90) | 4 (100) | |
Abbreviation: GC: glucocorticoid.
In this single-centre cross-sectional study of 44 patients with BS, we report a 13.6% prevalence of frailty and a 59% prevalence of pre-frailty based on the Fried frailty definition. Frail BS patients had higher CRP levels at diagnosis and during the study visit. In the frail group, the age of symptom onset and age of diagnosis was higher, and systemic GC use was higher when active drug use was evaluated. All patients using corticosteroids experienced at least one GC-related adverse event, but there was no significant difference in their cumulative frequency between patients by frailty classification. To the best our knowledge, this is the first investigation concerning the prevalence of frailty and its association with disease characteristics and GC use in patients with BS.
Over time, there has been a rise in research on the prevalence of frailty or pre-frailty in rheumatic patients; however, the majority of these studies have focused on RA patients.20 Pooled frailty and pre-frailty prevalence in this patient group were found to be 33.5% and 39.9%, respectively, in a recent systematic review.20 A weighted average prevalence of 9.9% was reported by a recent systematic review of 15 studies with 44,894 participants, utilizing physical frailty definitions. Pre-frailty had a weighted average prevalence of 44.2%, according to the same study.21 More recently, according to Tada et al.,22 there were 18.9%, 38.9%, and 42.2% prevalences of frailty, pre-frailty, and normal in RA patients. In RA cohorts, pre-frailty is more common (69%) than in geriatric cohorts (40–55%).23 In a cross-sectional study that determined the prevalence and clinical profile of frailty in 94 patients with systemic sclerosis (SSc), 28.7% of patients were evaluated as frail and 53 patients as 56.4% pre-frail according to the FRAIL scale.24 Patients with long-standing SSc were more likely to be frail, and this condition was linked to hospital admissions within the previous year, limitations in daily activities, and disability. There is a paucity of frailty in BS. Despite our sample size being relatively small, with a low comorbidity burden, and a relatively young average age, we found a higher prevalence of frailty and pre-fraility than reported for community-dwelling older adults. It may be suggested that people with inflammatory rheumatic disease may be more prone to frailty even in middle age.
Systemic inflammation is closely linked to fraility.25 High IL-6 and TNFα levels are associated with reduced muscle mass and decreased strength.26 Frailty, reduced functional ability, and decreased mobility are associated with higher levels of proinflammatory cytokines.5 There is evidence linking inflammatory markers like CRP and ESR to frailty, and there are also independent relationships between CRP and outcomes like mortality.5 In patients with inflammatory rheumatic diseases like RA, there has also been a reported correlation between frailty and elevated CRP levels.27,28 Patients who were already frail and pre-frail at time of diagnosis and at last visit had higher median CRP levels compared to normal patients. In the study evaluating the prevalence of frailty in polymyalgia rheumatic (PMR) patients, the prevalence of frailty and pre-frailty was 17% and 59%, respectively. At diagnosis, compared to pre-frail and robust patients, frail patients had higher levels of inflammatory markers, similar to our patient population.29 Elevation of CRP and other inflammatory markers can be pursued with ageing, including ageing-related disorders such as frailty.30 Elevated inflammatory markers in our study showed a stronger association with frailty than chronological age. Consequently, immunosuppressive medication could be very effective in preventing frailty. Further studies are needed on the extent to which increased inflammation predicts vulnerability at BS presentation and the role of baseline vulnerability in long-term health consequences.
In rheumatic diseases, frailty has been linked to physical function, gender, and disease activity; of these, disease activity was a significant predictor of frailty in RA.20 In a meta-analysis evaluating frailty in rheumatoid arthritis,20 which included 8556 patients, the disease activity were associated with the prevalence of frailty in RA patients. Katz et al.,31 used Fried's phenotype criteria in 2016 to evaluate frailty in 152 women with systemic lupus erythematosus (SLE) (mean age 48 years). Of the sample, 20% were classified as frail and 50% as pre-frail. The most frequently occurring variables were exhaustion, weakness, and inactivity (45%, 31%, and 29%, respectively). By frailty classification, there were no differences in age, race, education, duration of the disease, or history of smoking. Pre-frail and frail women used steroids at higher rates. There was a substantial worsening in ratings of disease activity, damage and pain as frailty state moved from robust, to pre-frail, to frail. In our study, disease activity BDCAF and damage index BODI scores were similar in frail and healthy patients.
Prolonged GCs treatment is estimated to be administered to 1%–2% of the population. GCs are used to treat a variety of diseases.32 Chronic steroid therapy can have a negative impact on muscle and bone, which can result in frailty.33 In our study, all patients reported experiencing glucocorticoid-associated adverse effects. Extended exposure to GCs raises the risk of osteoporosis, muscle atrophy, and cardiometabolic comorbidities.34 Nevertheless, little is known about the relationship between exposure to GCs and frailty. A recent study of older adults using a cumulative deficit definition of frailty (i.e. accumulation of age-related deficits) linked the use of GCs to an increased risk of frailty.35 Nevertheless, there was no correlation found with the Fried frailty phenotype's definition of frailty. Frailty and GC exposure have not been linked in rheumatic disease patients, and characteristics like disease activity or manifestations can make determining this relationship more difficult.
The most frequently encountered criteria in the original Fried study were inactivity, followed by weakness and slowness.19 Frequency of criteria in the PMR study was highest for weakness and exhaustion and lowest for slowness and inactivity.29 Similarly, in frail patients with RA and SLE, weakness and exhaustion have been frequently observed, but slowness has been observed less frequently.31,36 Although peripheral arthritis symptoms may affect the measurement of hand grip strength, it is important note that only a small minority of patients in our study (27%) had peripheral arthritis and 47% had arthralgia symptoms, with no statistical differences between groups, making it less likely that hand arthritis symptoms would affect hand grip assessment. In our study, exhaustion and weakness and were the most frequent criteria, while slowness was the least common criteria. When patients with underlying inflammatory conditions are compared, variations in the frequency of these criteria may bring attention to the ways in which these populations’ frailty processes differ.
The major strength of this study is that, it is the first study to investigate both frailty and pre-frailty status in BS patients. Our study is associated with several limitations in addition to small sample size. The first was the exclusion of data from a matched control group. Second, since we only included patients from one facility in our sample, it is impossible to extrapolate our results.
In conclusion, this single-centre cross-sectional study shows that both frailty and pre-frailty are commonly detected even in younger patients with BS. Inflammation can be described as potential determinants of frailty status. Acute and chronic inflammation, multiorgan involvement, gastrointestinal symptoms, and physical limitations due to musculoskeletal, cardiac, and pulmonary involvement are among the numerous reasons why patients with BS are more likely to become frail. Longitudinal studies are needed to identify patients with BS who are more prone to frailty or pre-frailty syndrome over time.
Authors’ contributionsAll authors provided final approval of the manuscript and revised it critically. Concept – H.A., S.C.G.; design – H.A., S.C.G.; supervision – B.A., H.A., S.C.G.; materials – H.A., H.B., S.C.G., B.A., E.K.E., R.K.U.; data collection and/or processing – H.A., H.B., S.C.G., B.A., E.K.E., K.O., R.K.U.; analysis and/or interpretation – H.A., H.B., S.C.G., B.A., E.K.E., K.O., R.K.U.; literature review – H.A., H.B., S.C.G., B.A., E.K.E., K.O., R.K.U.; writing – H.A., H.B., S.C.G., B.A., E.K.E., K.O., R.K.U.; critical review – H.A., H.B., S.C.G., B.A., E.K.E., K.O., R.K.U.
FundingNone declared.
Conflict of interestNone declared.


