





Osteoarthritis (OA) is the most prevalent articular disease worldwide, and its prevalence is highly variable depending on the classification criteria, population studied, and/or affected joints considered. Reporting epidemiologic data about clinical and radiological OA prevalence in Mexico has not been done before.
Patients and methodsA descriptive cross-sectional study was carried out with participants of Mexico City, and included both men and women above 40 years of age. All participants were evaluated with radiological and clinical criteria for OA.
ResultsTwo hundred and four individuals participated in the study: 80 men (39.2%) and 124 women (60.8%). The average age was 57.4±10.9 years. Using clinical criteria alone, 36 participants were found to have hand OA (17.6%; 95% CI, 13–23.4), 37 with hip OA (18.1%; 95% CI 13.4–24), and 40 with knee OA (19.6%; 95% CI 14.7–25.6). When radiological criteria were used, 51 individuals were reported as having hand OA (25%; 95% CI 19.5–31), 54 with hip OA (26.5%; 95% CI 20.8–32.9), and 52 with knee OA (25.5%; 95% CI 20–31.8). When clinical criteria were used and then corroborated with radiological criteria, the prevalence was 28 individuals with hand OA (13.7%; 95% CI 9.6–19), 31 with hip OA (15.1%; 95% CI 10.9–20.7), and 36 with knee OA 36 (17.6%; 95% CI 12.2–26.2).
DiscussionThe prevalences found in this study are greater than those found in other studies in Mexico that only report clinical criteria.
La osteoartritis (OA) es la enfermedad articular más prevalente a nivel mundial; la prevalencia reportada es muy variable ya que depende de los criterios de clasificación, la población estudiada y/o las articulaciones afectadas. Previamente no se habían reportado datos epidemiológicos sobre la prevalencia clínica y radiológica de la OA en México.
Pacientes y métodosSe realizó un estudio descriptivo y transversal, se incluyeron participantes de cualquier sexo mayores de 40 años de la Ciudad de México, todos ellos fueron evaluados con criterios radiológicos y clínicos para la OA.
ResultadosSe analizaron 204 individuos, 80 varones (39,2%) y 124 mujeres (60,8%). La edad promedio fue de 57,4±10,9 años. Usando solo criterios clínicos, 36 participantes tuvieron OA de mano (17,6%, IC 95%, 13–23,4), 37 con OA de cadera (18,1%, IC 95% 13,4–24) y 40 con OA de rodilla (19,6% IC 95% 14,7–25,6). Cuando se utilizaron los criterios radiológicos, se informó que 51 individuos tenían OA de mano (25%: IC 95% 19,5–31), 54 con OA de cadera (26,5% IC 95% 20,8–32,9) y 52 con OA de rodilla (25,5%; IC 95% 20–31,8). Al utilizar criterios clínicos y luego corroborados por criterios radiológicos, la prevalencia fue de 28 individuos con OA de mano (13,7% IC 95% 9,6–19), 31 con OA de cadera (15,1% IC 95% 10,9–20,7) y 36 con OA de rodilla 36 (17,6%; IC 95% 12,2–26,2).
DiscusiónLas prevalencias encontradas en este estudio son mayores a las encontradas en otros estudios en México que solo reportan criterios clínicos.
Osteoarthritis (OA) is a multifactorial joint disease that represents a group of pathologies with clinical manifestations and common morphological and radiological changes.1 OA is the most common joint disease and the leading cause of disability in adults above 60 years of age.2
The reported prevalence of the disease is variable, ranging from 1%–2% to >80%, depending on the classification criteria, population studied, and/or affected joints considered.3,4
For epidemiological purposes, OA can be classified according to clinical or radiological methods. Clinical classification of OA is based on the presence of pain, either self-reported or upon physical examination of the joint, along with other findings during the physical examination and/or patient interview. The most commonly used clinical classification criteria are those proposed by the American College of Rheumatology (ACR).5–7 Radiological classification is based mainly on the presence of osteophytes, narrowing of the articular space, and bone sclerosis; the most common radiological criteria employed are those proposed by the World Health Organization (WHO), which are based on the Kellgren–Lawrence (KL) classification.8
It is widely accepted that there is no high correlation between clinical manifestations and radiological alterations, although in clinical practice the diagnosis of OA is performed utilizing the clinical findings corroborated with the radiological exam.9
OA may develop in any diarthroidal joint, but the most commonly affected of these are knees, hips, and hands.10 In Mexico, information on OA prevalence derives from surveys, such as the National Survey on Health and Nutrition (ENSAUT) or “The Community Oriented Program for the Control of Rheumatic Diseases” (COPCORD), neither of which includes information on radiographic findings.11–14
The objective of this study was to describe the clinical and radiological prevalence of hip, knee, and hand OA in an adult population in Mexico City.
Patients and MethodsA descriptive cross-sectional study was carried out. The study protocol was registered in Mexico City's Secretariat of Health, as well with the National Institute of Rehabilitation's “Luis Guillermo Ibarra Ibarra”, one of Mexico's National Health Institutes. The Secretariat of Health registration number was 101-011-04-13 and the internal Research Committee number was 08/12.
The study was performed at three primary care clinics belonging to the Mexico City's Secretariat of Health; however, the sample was not taken from patients of the clinics, but from people accompanying patients. The participants were questioned about the reason for visiting the clinic and in all cases it must be only to accompany patients. All primary care are clinics, are part of the Mexican public health system, and are open to all the population.
All participants were individuals of both genders, >40 years of age, and all classified as mexican-mestizo, by questioning on having two previous generations of parents and grandparents born in Mexico. In order to avoid selection bias, participants were excluded if they were a first degree family member of a patient previously known with OA; to avoid cases of familiar OA; or persons with a history of joint surgery (secondary OA); also pregnant or nursing women were excluded.
The sample was not obtained in a random or stratified manner, so the prevalence found represents the areas of the chosen clinics (Tlalpan, Coyoacán and Gustavo A. Madero municipalities) which together represent a population of 2413733 inhabitants according to the 2010 national population census, and approximately 34% are older than 40 years.
All participants were chosen, for convenience, in consecutive order as they arrived at the primary-care clinic. These individuals were invited to participate in the study. Those who accepted signed an informed consent and had a clinical interview at that time including socio-demographic data, and risk factors for OA; a physical examination that comprised height and weight measurement, exploration for pain, movement, alignment, and joint crepitus. The clinical examination was performed by a Physical Medicine and Rehabilitation Specialist, expert in orthopedic conditions, and it was done on the participant's non-dominant side or on the symptomatic side if symptoms were present.
Simple plain X-rays were then performed on the same side as the examination; anterio-posterior projection was used for hip; standing anterior–posterior and lateral projections for knee, and anterior–posterior and oblique projections for hand.
Participants were categorized as either with or without knee, hip, or hand OA according to ACR clinical criteria and to the Kellgren–Lawrence radiological classification. For clinical classification of knee OA, knee pain and at least three of the following proposed criteria (age >50 years, morning rigidity <30min, crepitus when moving the joint, bone sensitivity, bone growths, or non-palpable heat at a synovial level) were utilized.5 For hip OA classification, participants should present either localized pain or limited movement in the internal hip rotation by at least 15°, and hip flexion of <115°, or localized pain in internal rotation in addition to morning hip rigidity lasting <60min and age above 50 years;7 for classification of hand OA: pain; discomfort, and/or rigidity and at least three of the following: bone growth in two or more of the 10 selected joints; fewer than three inflamed metacarpophalangeal joints; bone growth in two or more distal interphalangeal joints, and deformity of at least one of the 10 selected joints.6
All radiographies were evaluated by an independent physician (non-radiologist) trained and expert in musculoskeletal radiology, who was blinded to the clinical classification. The Kellgren–Lawrence classification of grades 0–IV was used as follows: grade 0 in the absence of radiographic signs of OA; grade I, uncertain joint space narrowing and the possible presence of osteophytes; grade II, definite osteophytes and narrowing of joint space; grade III, osteophytes, important narrowing, subchondral sclerosis, and possible bony deformity, and grade IV, multiple osteophytes, marked narrowing of the space, severe sclerosis, and definitive bony deformity.8
Grades 0 and I were considered normal and from II to IV were considered positive for radiological OA.
Another data obtained from subjects was: tobacco consumption, alcohol consumption, repetitive trauma in a joint, previous fractures, current and previous exercise performance, comorbidities, pain site, joint mobility limitations, and risk occupations for OA.
Sample SizeSample size was calculated according to the formula for prevalence studies for a single proportion, with a 5% margin of error and a 95 confidence Interval (95% CI). Assuming that the general prevalence of OA in Mexico City is 12.8%14 and an unknown population size, the total sample size was calculated as 172 individuals.
Statistical AnalysisDescriptive statistical analysis was performed to summarize the data. Prevalence was reported as frequencies and percentages, with their 95% CI. To make statistical inferences about epidemiological variables, a Student's t-test was performed for quantitative variables and χ2-test was performed for qualitative variables. Alpha level was 0.05. IBM SPSS Statistics Base Ver. 22.0 software was used for calculations.
ResultsTwo hundred and thirty-four individuals accomplished the inclusion criteria and were asked to participate: 30 of them refuse to do it because of the lack of time to stay in the clinic.
A total of 204 individuals were included in the study, and the demographic characteristics are shown in Table 1.
Demographic Characteristics.
| Demographics, n=204 | |
|---|---|
| Gender | |
| Female: n (%) | 124 (60.8) |
| Male: n (%) | 80 (39.2) |
| Age (years): mean±SD | 57.4±10.9 |
| Range | 42–86 |
| Age groups: n (%) | |
| 40–50 years | 71 (34.8) |
| 51–60 years | 64 (31.4) |
| 61–80 years | 64 (31.4) |
| >80 | 5 (2.4) |
| Body mass index (kg/m2): mean±SD (range) | 27.89±4.44 |
| Range | 18.1–37.2 |
| Normal: n (%) | 57 (27.9) |
| Overweight: n (%) | 79 (38.3) |
| Obesity: n (%) | 68 (33.3) |
| Current tobaco comsumption: n (%) | 82 (40.2) |
| Lifetime use (months): mean±SD | 20.6±15 |
| Alcohol comsumption: n (%) | 34 (16.7) |
| Lifetime use (months): mean±SD | 20.77±13.27 |
| Current exercise practice: n (%) | 52 (25.5) |
| Time per week (minutes): mean±SD | 132.5±28.4 |
| Comorbilities | |
| Hypertension: n (%) | 52 (25.5) |
| Type 2 diabetes: n (%) | 30 (14.7) |
| Cancer: n (%) | 4 (0.1) |
| Occupational risk for OA | |
| Hand: n (%) | 75 (36) |
| Hip: n (%) | 44 (21.5) |
| Knee: n (%) | 51 (25) |
Calculating prevalence with clinical criteria alone, 36 participants were found to have hand OA (17.6%; 95% CI, 13–23.4), 37 with hip OA (18.1%; 95% CI, 13.4–24), and 40 with knee OA (19.6%; 95% CI, 14.7–25.6).
When radiological criteria were utilized, 51 individuals had hand OA (25%; 95% CI, 19.5–31), 54 had hip OA (26.5%; 95% CI, 20.8–32.9), and 52 had knee OA (25.5%; 95% CI, 20–31.8).
When clinical criteria were employed and subsequently corroborated with radiological criteria, prevalence was 28 individuals with hand OA (13.7%; 95% CI, 9.6–19), 31 with hip OA (15.1%; 95% CI, 10.9–20.7), and 36 with knee OA 36 (17.6%; 95% CI, 12.2–26.2).
Prevalences by gender are shown in Table 2, and by age groups in Table 3.
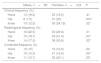
Prevalence Differences by Gender.
| Males, n=80 | Females, n=124 | P | |
|---|---|---|---|
| Clinical frequency (%) | |||
| Hand | 13 (16.2) | 23 (18.5) | .41 |
| Hip | 6 (7.5) | 31 (25) | .001* |
| Knee | 10 (12.5) | 30 (24.19) | .02* |
| Radiological frequency (%) | |||
| Hand | 18 (22.5) | 33 (26.6) | .31 |
| Hip | 15 (18.7) | 39 (31.4) | .03* |
| Knee | 14 (17.5) | 38 (30.6) | .02* |
| Combined frequency (%) | |||
| Hand | 12 (15) | 16 (12.9) | .52 |
| Hip | 10 (12.5) | 21 (16.9) | .05* |
| Knee | 11 (13.7) | 25 (20.1) | .05* |
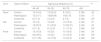
Prevalence Differences by Age Group.
| Joint | Type of criteria | Age-group frequency (%) | P | |||
|---|---|---|---|---|---|---|
| 40–49 | 50–59 | 60–79 | >80 | |||
| Hand | Clinical | 12 (16.9) | 13 (20.3) | 8 (12.5) | 2 (40) | .42 |
| Radiological | 15 (21.1) | 19(29.68) | 14(21.8) | 3 (60) | .17 | |
| Combined | 8 (11.2) | 8 (12.5) | 9 (14) | 3 (60) | .05* | |
| Hip | Clinical | 10 (14) | 15 (23) | 10 (15.6) | 2 (40) | .27 |
| Radiological | 18 (25.3) | 21 (32.8) | 13 (20.31) | 2 (40) | .32 | |
| Combined | 9 (11.2) | 8 (12.5) | 11 (17.8) | 3 (60) | .03* | |
| Knee | Clinical | 13 (18.3) | 15 (23) | 10 (15.6) | 2 (40) | .34 |
| Radiological | 24 (33.8) | 16 (25) | 10 (15.6) | 2 (40) | .05* | |
| Combined | 8 (11.26) | 10 (15.6) | 14 (21.8) | 4 (80) | .02* | |
Bivariate analysis between the groups of patients with and without a clinical diagnosis of OA revealed statistically significant differences in variables such as BMI with hand OA (P=.03), with hip OA (P=.01); and with knee OA (P=.001); repetitive joint trauma with hand OA (P=.04) and with knee OA (P=.05), and with history of playing a sport with knee OA (P=.017). With radiological diagnosis, BMI was associated with hand (P=.05), hip (P=0.001), and knee (P=.01) OA, and repetitive joint injury, with hand (P=.03) and knee (P=.05) OA.
The results of radiologic grades are presented in Table 4.
DiscussionTo our knowledge, this is the first OA study in Mexico utilizing both clinical and radiological diagnostic criteria to determine OA prevalence. This is a more reliable evaluation of the disease and corroborates its elevated prevalence, highlighting the importance of OA in a Mexican population.
In this group of participants above the age of 40 years, the prevalence of OA in the three studied joints employing clinical criteria alone reached approximately 20%, while prevalence of OA utilizing radiological criteria was higher, around 25%. Upon combining both classification criteria, prevalence is reduced, with higher prevalence in knees, with 17.6%, followed by hips with 15.1%, and hands, with 13.7%.
Our findings show that the combination of both criteria more adequately adjusts prevalence, perhaps because they include the physiopathological changes in the disease (morphological changes in the joint) and the presence of symptoms.19
Our findings differ from those reported by Cardiel et al., who demonstrated a prevalence of OA at any site of 2.3% in general population in central Mexico, using the Community Oriented Program for Control of Rheumatic Diseases (COPCORD) survey, and according to this same study, in individuals >50 years, the authors found the prevalence of OA to be 11% (in any joint), which is lower than the prevalence that we found.11 Another Mexican study that used the same COPCORD methodology to report prevalence in five Mexican regions found an overall prevalence of clinical OA of 10.5%.14
The Framingham Study also took into account clinical and radiologic data. This study found prevalence of hand OA in individuals >26 years of age to be 6.8%: 9.2% in females and 3.8% in males. Our study found nearly double that, with hand OA as 13.7%, 15 and 12.9% in females and males, respectively, and hip OA as 15.1%, 16.9 and 12.5% in females and males, respectively. However, the Framingham Study population was considerably younger than ours.15
Another study derived from the Framingham Cohort reports knee OA prevalence with combined criteria to be 4.9% in adults over 26 years of age and 6.7% in adults aged over 45 years. Once again, the prevalences found in this present study are higher than those in the previous study.16,17 The Johnson County OA Project found knee prevalence in adults >45 years to be 16.7%,18 and hip OA prevalence to be 9.2%, prevalences in line with what we have reported in this current study.19
Other studies that have found similar prevalences to those reported by our research group,20 using only radiological criteria for knee OA include Hochberg in the US 30.4%,21 Odding in the Netherlands 24%,22 Shiozaki in Japan 21.9%,23 and Khang in China, 34.1%.24 Employing only clinical criteria for knee OA, Sudo in Japan found prevalence to be 21.2%,25 and Kim in Korea, 24.2%.26 Utilizing only radiological criteria to diagnose hip OA, Odding in the Netherlands reported prevalence at 15.2%,22 Cvijetiae in Croatia 23%,27 and Quintana, using clinical criteria, found a prevalence of 7.4% in Spain.28 It is important to bear in mind that the heterogeneity present in these previous studies is probably due to differences in methodology, type of population, sample size, and classification criteria.4
Regarding previously described risk factors for OA, the results of this study show a statistically significant association between OA, and age, gender, BMI, and repetitive joint injury, in line with what has been widely reported in the literature. In Mexican population, Arellano-Pérez et al. previously reported in a case–control study that age and menopause are major risk factors for knee OA, and tobacco consumption a protective factor, those findings were not corroborated by us, except by the age.29 However, other factors, such as occupation, physical activity, and exercise, despite being described as risk factors, were not shown to be statistically significant in our study.1,20 In the current study, occupational risk factors were not shown to influence prevalence. This is in contrast with other studies, in which these have been described as a major risk factor for OA.30 However, we must take into account that this study does not possess the methodological design for detecting risk factors and that the sample size was small and did not systematically evaluate occupational risks.
In our study, we found that the prevalence of OA rose significantly with age. This increase is particularly consistent when both clinical and radiological criteria are taken together, from 10%–15% at 40–50 years group to 60%–80% in the >80 years group. However, a slight decrease was found in the group aged between 61 and 80 years in comparison with the previous age group when clinical and radiological criteria are each taken separately. Upon combining both criteria, prevalence increased chronologically with age, with statistically significant differences observed between age groups, as has been widely described in the literature.1,30 The age group of participants above 80 years was observed to have a dramatic increase in prevalence, although this information should be taken with caution, as this group was composed of only five individuals.
In accordance with other studies, we found higher prevalence in females than in males; however, these differences were only in knee and hip OA, but not in hand; the difference is wide when only clinical criteria is taken, in hip is 25 vs 7.5% in women vs men, and in knee 24 vs 12.5%; the same pattern is observed with radiological criteria 31 vs 18% in hip and 30 vs 17% in knee, which shows a wide difference of gender-related prevalence of hip and knee OA in females. Although an increased prevalence of hand OA was observed in females in comparison to males, it did not reach statistically significant differences.
In our sample, for people with radiological OA diagnosis, the most common grade was II between 12 and 17%, although 4%–5% of our patients had grade IV, depending on the site, which reveals an elevated prevalence of OA in relation to early radiological grading.
OA affecting the hand, hip, and knee is a disease entertaining a high prevalence in this population. The results obtained in this study provide data that coincide in general with those reported in the international literature, although this study demonstrates a higher prevalence than that reported in other studies in Mexico. Our data allow for a more reliable definition of the epidemiology of this disease. Because OA is a common joint disease, better knowledge of its prevalence will permit the establishment of prevention policies and early detection strategies to avoid the disability generated by this entity.
Study LimitationsThe main limitation of the study is related to the sample selection, because it was not obtained from general population or in a probabilistic manner, and it is not representative of the whole population, or all Mexico City, and this could induce a selection bias; another limitation relies in the relatively small sample size, compared with other epidemiological studies and that the sample was not stratified by age, what difficult to make inferences on specific prevalence by age. It is necessary to carry out a study with a national sample, using both clinical and radiological criteria, to observe the prevalence throughout the entire country, because of the important prevalence variations in different geographical areas.
Conflict of Interests and Sources of FundingAll authors declare not having any conflict of interest in regard to this research. All resources were obtained from the Local and Federal Government through the Mexican Secretariat of Health.
We acknowledge the Secretariat of Health of Mexico City; Dr. Federico Lazcano Ramírez, President of the Investigation Commission; Dr. Francisco Osuna Sánchez, Dr. Martha Esthela Mandujano, and Dr. Fernando Rey Monroy, Directors of the Primary-care Centers, and all of the personnel of Gustavo A. Madero, Coyoacán, and Tlalpan Primary-care Centers for their greatly appreciated support of and collaboration with our team.


