



Spondyloarthropaties (SpA) are a group of chronic inflammatory rheumatic diseases that include ankylosing spondylitis (AS), psoriatic arthritis (PsA) reactive arthritis (ReA), spondyloarthritis associated with inflammatory bowel diseases (IBD) and undifferentiated spondyloarthropaties (U-SpA)1. Although each of these entities has specific characteristics they do share some clinical, radiologic and genetic manifestations.
The main common feature of SpA is back pain due to spinal inflammation (spondylitis and/or sacroiliitis). Other common characteristics are peripheral arthritis, usually oligoarticular affecting lower limbs, enthesitis and extra-articular involvement (acute anterior uveitis, inflammatory bowel lesions and psoriasis)2.
As opposed to other rheumatic diseases like Rheumatoid Arthritis, the incidence and prevalence of SpA is not well known and in Portugal this data is not available. The clinical course and prognosis of SpA is diverse due to the group heterogeneity but also to different clinical presentations with each disease3.
In AS the age of disease onset is around the second or third decade4, but in the other subtypes of SpA it's not possible to define a risk period for the development of the disease.
Although SpA classically have been described as affecting more males than females4, it is now beginning to be accepted that its prevalence may be similar in both genders. Despite this controversy it is more or less consensual that some clinical forms are more common in males while other subtypes affect equally both or are more common in females. The genetic influence in the development of these diseases, evidenced by a prevalence of HLA-B27 allele in Spa patients that ranges between 50 and 95%, is reflected in a trend to familiar association, which is recognized in multiple epidemiologic contexts5,6.For historical reasons, the Ibero-american countries share many characteristics. We decided to participate in the RESPONDIA group with the purpose of discovering the similarities and the differences between these countries concerning the genetic, clinical and socioeconomic aspects of spondyloarthropaties.
The objective of this work is to give a descriptive analysis of the main characteristics of the Portuguese patients with spondyloarthropaties included in the RESPONDIA study.
Material and methods
This was an observational and transversal study that included patients recruited from 4 Portuguese Rheumatology Departments (Instituto Português de Reumatologia, Lisboa; Hospital de Santa Maria, Lisboa; Centro Hospitalar Lisboa Ocidental - Hospital Egas Moniz, Lisboa e Hospital Infante D. Pedro, Aveiro), between June 2007 and March 2008. All the data was registered in the REGISPONSER (Registro de Espondioartropatías de la Sociedad Española de Reumatología) online database7. The general methodology, including inclusion criteria, study variables, online database development and data analysis are described in other article published in this journal8. Patients that were included fulfilled the European Spondyloarthropaties Study Group (ESSG) classification criteria9 or the Amor criteria10.
Portugal characterization
Portugal is a country located in the southwest of Europe, situated in the western part of the Iberian Peninsula as well as in North Atlantic archipelagos. Its total surface area is 92,391 km2 and it is the most occidental nation of the European continent. The Portuguese Gross Domestic Product (GDP) is of $253,557 billions USD a year and the GDP per capita (estimation of 2006) of $27,621USD a year.
On 31st December 2006, according to the Portuguese National Statistic Institute11, the resident population was estimated at 10 599 095 people, of which 5 129 937 are male and 5 469 158 female. 15.5% are children (0-14 years old); 67.3% are of working age (15-64 years old), 17.5% are older than 65 years and people older than 75 years represent 7.7% of the total population. According to the United Nations Children's Fund (UNICEF) report: "The state of the world's children 2007"12, Portugal is ranked 13th among more than 180 countries with the lowest child mortality rate. The report also notices that Portugal is one of the countries with the highest like expectancy in the world, 78 years.
Nowadays there are around 550 thousand immigrants living in Portugal, which represents approximately 5% of the whole population, most of them being from Brazil (66,700), Ukraine (65,800) and Cape Verde (64,300), between other countries, such as Moldavia, Romania, Guinea-Bissau, Angola, East-Timor, Mozambique, Saint Tome and Principe and Russia11.
The majority of the Portuguese population is white. The literacy rate (older than 15 years that know how to read and write) is of 93.3% (95.5% for males and 91.3% for females)13.
In Portugal health is a constitutional right. The health system is almost exclusively supported by the government, which has its own primary and secondary care structures.
Results
110 patients with the diagnosis of SpA (59 males [58.4%] and 42 females [41.6%]), and with a mean age of 46.5 ± 12,9 years, were included. Socio-demographic characteristics of this population are described in table 1. The most common diagnosis among SpA was Ankylosing Spondylitis (AS) followed by Psoriatic Arthritis (PsA) (fig. 1).


Figure 1.SpA. Subtypes.
The mean age of disease onset was 26.7 ± 10.9 years being before the age of 18 in 19% of patients while in 40% the first symptoms started between the age of 21 and 30. The diagnosis was established before the age of 18 in only 2% of patients. The majority of patients were diagnosed between the age of 21 and 30 (34%) and between the age of 31 and 40 (26.8%) The delay in the diagnosis was longer than 10 years in 25.5% of the patients.
The most common initial manifestation was lower back pain in 63.4% (table 2). The axial involvement was more frequent (50.5%) followed by the association of peripheral arthritis and axial symptoms (47.5%). Lower limb joints were more affected than upper limb joints. With regard to extra-articular manifestations acute anterior uveitis and dactilitis were the most common (34% and 7.9% of patients, respectively) (table 3).


Previous family history of spondyloarthropaties was identified in 29 patients (29.9%).
The majority of patients (94.8%) had previously taken non-steroidal anti-inflammatory drugs (NSAIDs): 55.2% daily and 39.6% on demand, and also corticosteroids in 29%. The disease-modifying antirheumatic drugs (DMARDs) most used were sulfasalazine (47.3%) and methotrexate (23.1%). Only 10.8% of patients had previously been prescribed TNF alpha blockers agents (fig. 2).

Figure 2.Previous prescribed treatments.
The results of the medical physical observation and applied questionnaires were very diverse. The mean Bath ankylosing spondylitis disease activity index (BASDAI) was of 4.2 cm and the mean Bath ankylosing spondylitis disease functional index (BASFI) was of 3.6 cm.
The HLA B27 was positive in 34 patients (85%) and negative in 6 (15%). In 61 patients this information was not available.
Results of the ankylosing spondylitis group
85 patients were included, mainly male (59%) with a mean age of disease onset of 26 ± 11.3 years and mean disease duration of 1.8 ± 0.9 years. The delay in the diagnosis was of 1 to 5 years in 35 patients, 6 to 10 years in 13 and more than 10 years in 25 patients. The axial involvement was predominant (54%) while the combination of axial and peripheral arthritis was verified in the remaining patients (46%). Low back pain was the most frequent complaint (97.6%). Asymmetric arthritis of the lower limbs was referred to in 42.3% and enthesitis in 35.3% of patients.
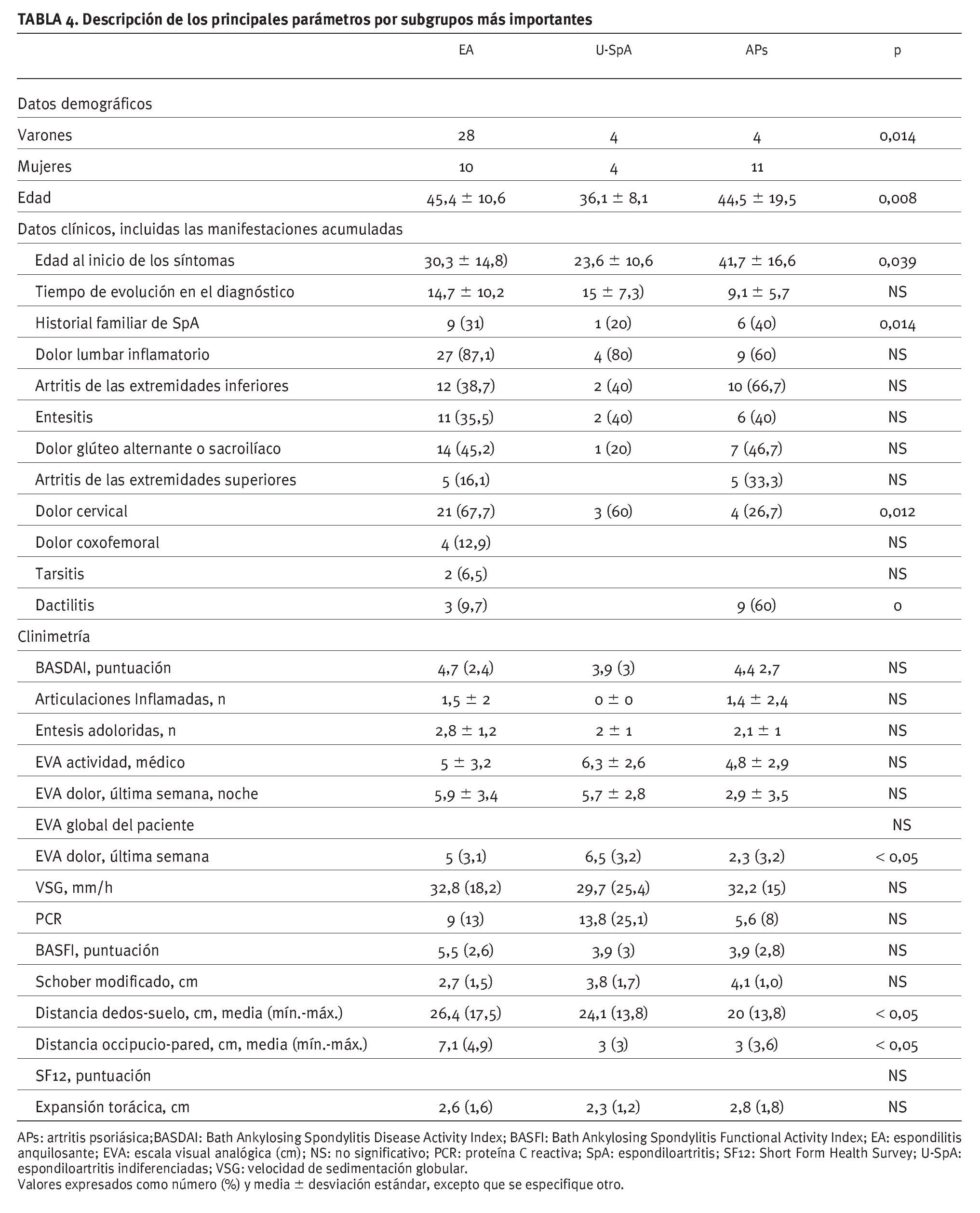
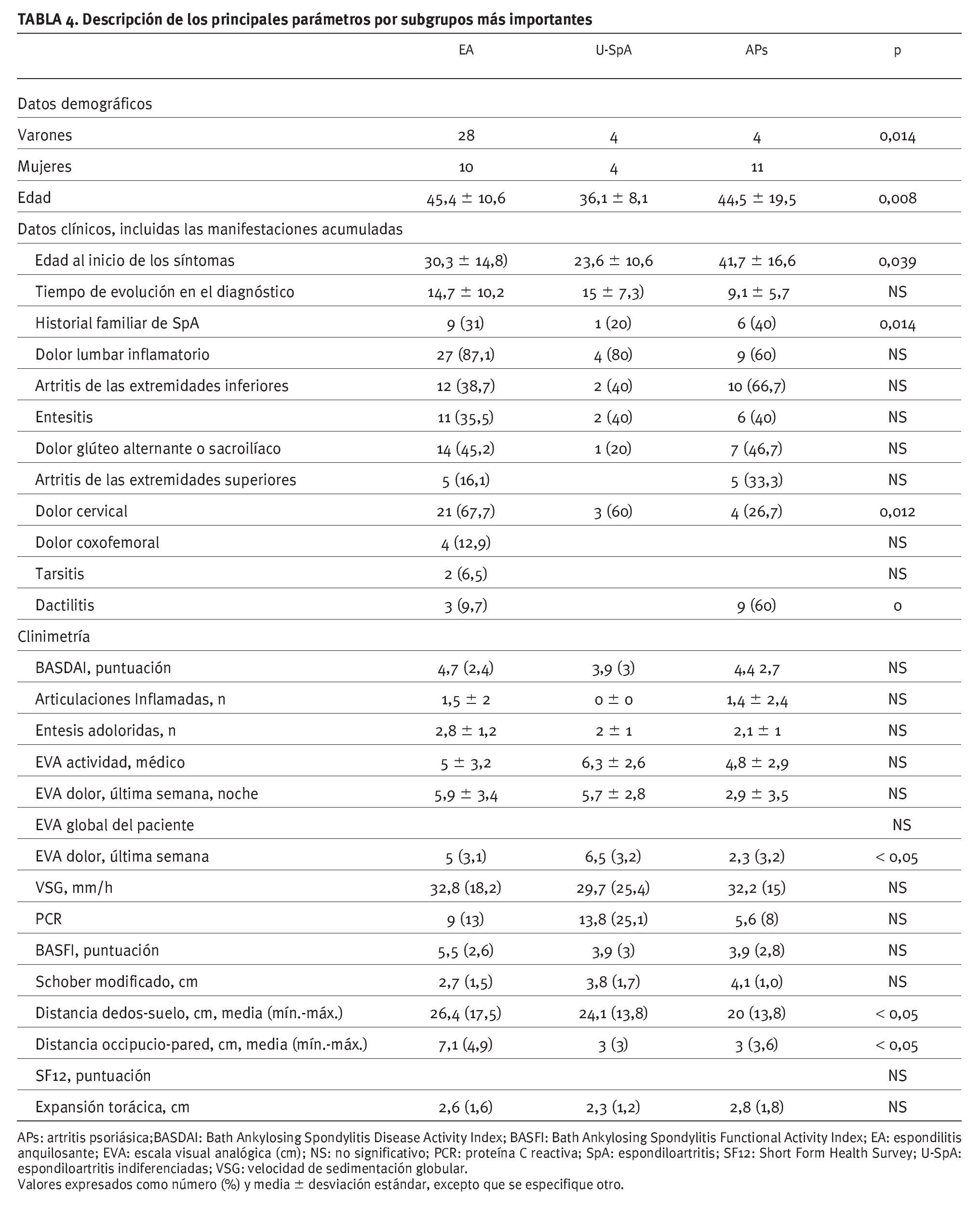
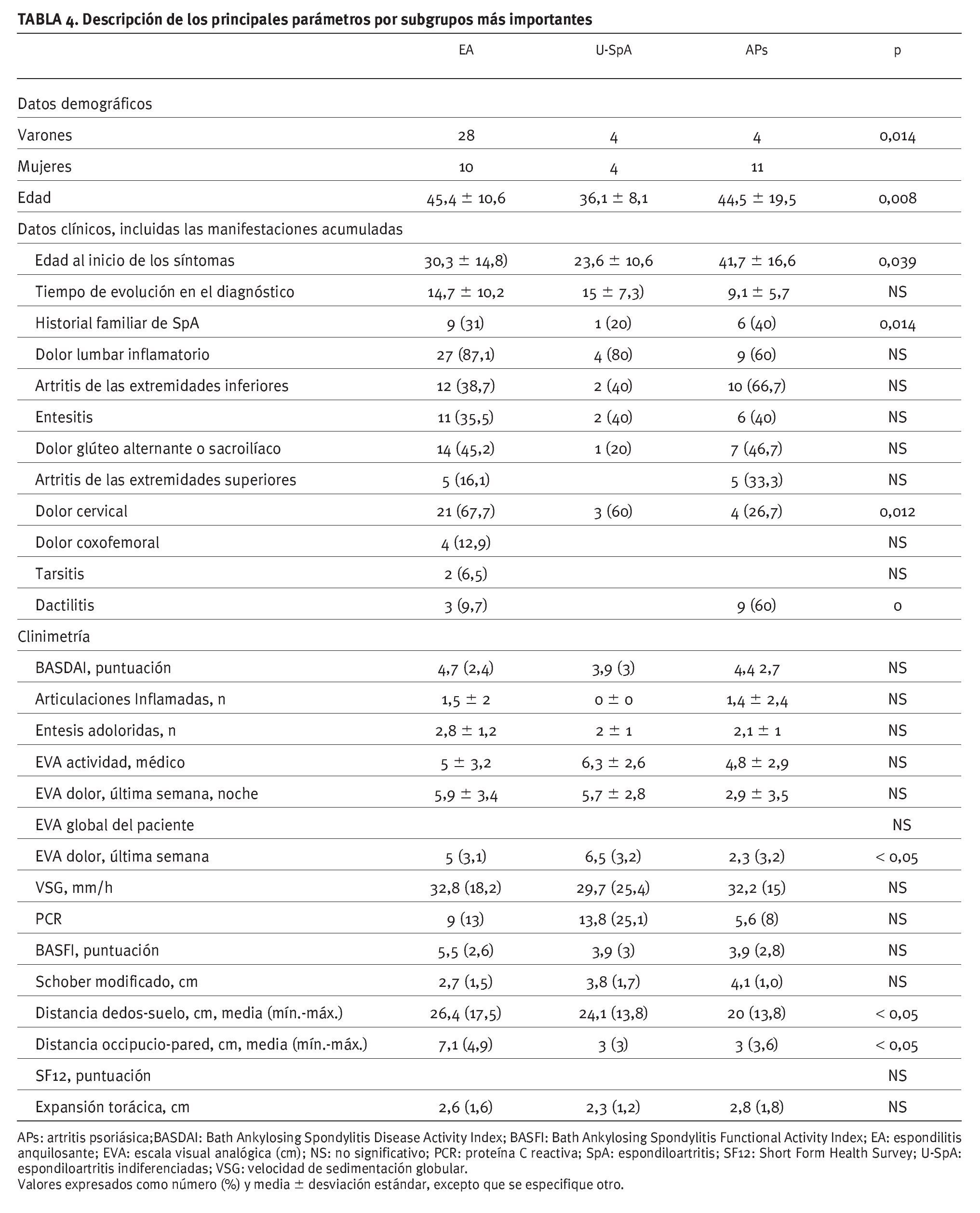
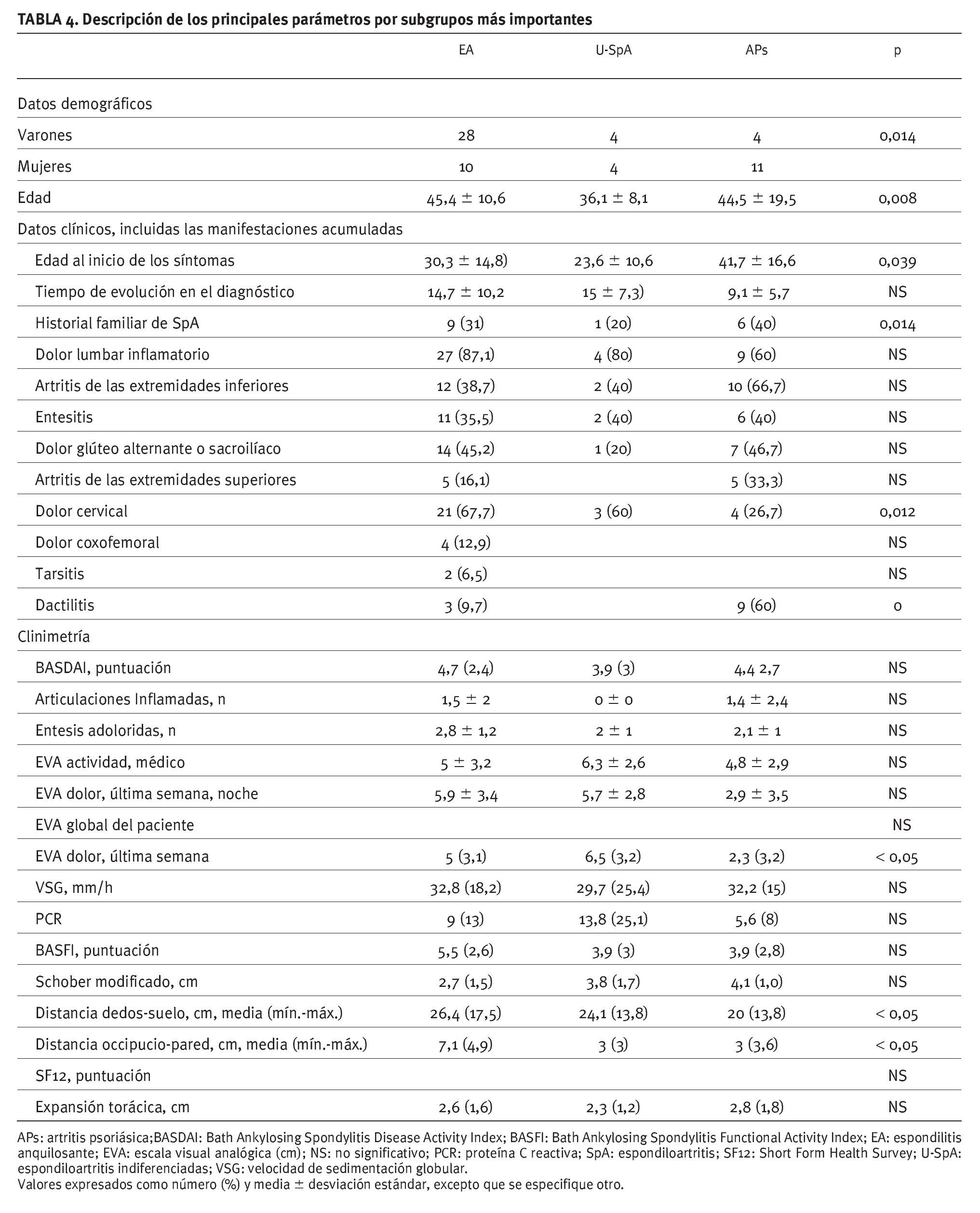
Acute anterior uveitis was the most common extra-articular manifestation (36.5%) (table 4).

The majority of patients (88.8%) were taking NSAIDs (46.3% daily and 42.5% on demand) and 19.5% were undergoing cortisteroids. Concerning DMARDs, 38.5% patients were using sulfasalazine, methotrexate by 22.1% patients and TNF alpha blockers by 11.8% patients. None of them were taking leflunomide.
There was not a history of previous genitourinary, intestinal or respiratory infections in any of the patients. 27 patients had family history of spondyloarthropaties. 8 patients had undergone hip replacement surgery. The mean BASDAI in this group was 4.1cm and the mean BASFI 3.7cm. 13 patients were incapable of work (11 permanently and 2 temporarily). HLA B27 was positive in 85.7% patients, negative in 14.2% and it was not known in 50 patients.
The other subtype groups (Psoriatic arthritis, Reactive arthritis, Spondyloarthritis associated with inflammatory bowel diseases and Undifferentiated spondyloarthritis included few patients not allowing an individual characterization.
Conclusions
In this group of portuguese patients ankylosing spondylitis was the most frequent subtype of spondyloarthropaty. Males were predominantly affected which is according to the literature data14. The mean age of disease onset was also similar to that found in the literature. The axial involvement was the most common and the acute anterior uveitis the most frequent extra-articular manifestation. Contrary to what is described in other countries, namely in Mexico15, tarsitis in not a common characteristic in AS Portuguese patients. 13 of these patients were incapable of work with significant socioeconomic consequences. Sulfasalazine was the most used DMARD while leflunomide was never prescribed. NSAIDs are still the most common drugs used to treat AS. Although the BASDAI score is higher than 4, there was only a small number of patients (n=10), were undergoing TNF alpha blocking agents.
The high number of AS patients treated with corticosteroids (n=24) is probably related to its used to treat acute anterior uveitis (n=31). This study has many limitations including the small number of patients, the methodology for data collection without previous inter and intra investigator analysis.
Acknowledgments
The Portuguese RESPONDIA group would like to thank Prof. Eduardo Collantes-Estevez for all the unconditional support given to this project from day one and also to the Portuguese Rheumatology Society. This group also thanks Dra. Pilar Font for the development of the database, and Dra. Janitzia Vázquez-Mellado for the coordination and analysis of patients' data.
Correspondence:
Dra. A. Barcelos.
Unidade de Reumatologia. Hospital Infante D. Pedro. Av Artur Ravara. 3814-501 Aveiro. Portugal.
E-mail: barcelos.a@clix.pt


