
IgG4 related diseases (IgG4-RD) are characterized mainly by organic dysfunction and inflammation with lymphoplasmacytic cells infiltration.
MethodsWe conducted a retrospective study. We analyzed patients with a diagnosis of IgG4-RD through histopathologic registries. We divided the study into three phases: (i) extraction of data from the registries of the Pathology Department, including specimens reported with: non-specific inflammation with plasmatic cell infiltration, inflammatory pseudo-tumors and storiform fibrosis, and excluding any report of cancer or infection; (ii) from the selected specimens, three pathologists microscopically re-analyzed these biopsies and included only those who had at least two of the inclusion criteria cited above; (iii) finally, immunostaining was performed in the specimens selected in the second phase. The selected biopsies were cataloged as compatible for IgG4-RD if they had at least 3 inclusion criteria and as probable if they had 2 inclusion criteria.
ResultsOn the first phase of the study we analyzed 23,720 biopsies, from which we included 71 and excluded 29 specimens; the rest of the specimens (n=41) underwent immunostaining. From the biopsies included, 41.4% (n=17/71) were positive to IgG4, with the most common histological diagnosis for the positive specimens being granulomatous mastitis, which represented 12.1% of the specimens cataloged initially as probable. The rest of the positive biopsies were from aortitis, dacrioadenitis and/or sialoadenitis, lung pseudo-inflammatory tumor, pericarditis and chronic pancreatitis.
ConclusionsThe suspicion of IgG4 related disease should not be based solely on clinical manifestations or serology. In the present study we confirm the characteristic changes of IgG4-RD in patients without initial clinical suspicion.
Las enfermedades relacionadas con IgG4 (ER-IgG4) se caracterizan por inflamación y disfunción orgánica asociadas a células plasmáticas productoras de IgG4.
MétodosAnalizamos pacientes con ER-IgG4 de acuerdo con: a)búsqueda de resultados en la base de datos de Patología con: reacción inflamatoria inespecífica con infiltrado linfoplasmocítico, pseudotumores inflamatorios y fibrosis estoriforme; b)análisis microscópico de biopsias con criterios de inclusión de la primer fase, y c)inmunohistoquímica de biopsias seleccionadas en la segunda fase.
ResultadosEvaluamos en la primera fase 23.720 biopsias, y a 41/71 que reunieron los criterios de inclusión les realizamos inmunohistoquímica para IgG4. El 41,4% de estas tuvieron IgG4+, y el diagnóstico histológico más frecuente asociado fue mastitis granulomatosa (12,1% de muestras catalogadas inicialmente como probables). El resto incluyeron reportes de aortitis, dacrioadenitis o sialoadenitis, pseudotumor inflamatorio pulmonar y pancreatitis crónica.
ConclusionesLa sospecha de enfermedades relacionadas con IgG4 no debe basarse únicamente en manifestaciones clínicas distintivas o solo en serología. Nuestro estudio incluye pacientes con ER-IgG4 sin sospecha clínica inicial.
Attention has recently been focused on the importance of multiorgan disorders characterized by the formation of inflammatory pseudotumors, with or without organ dysfunction, accompanied by increased immunoglobulin G4 (IgG4) levels.1
IgG4-related disease (IgG4-RD) consists of infiltration by plasma cells responsible for IgG4 synthesis and secretion. The diagnostic criteria are characterized by: clinical manifestations that vary depending on the affected organ and serological and histopathological findings. It is associated with a wide range of clinical signs, and the disease characteristically involves the exocrine glands (lacrimal and salivary glands and pancreas); however, it has been described as being practically universal as it can affect nearly any organ.2–6 The serological diagnosis is based on high IgG4 levels (≥135mg/dl); however, this criterion is not absolute, as we find patients in whom this immunoglobulin subclass is not elevated despite their confirmed diagnosis; moreover, increased IgG4 levels have been reported in other diseases.7 The diagnostic criterion having the greatest specificity is the histological examination. Thus, it is necessary to demonstrate that the histopathological criteria for the disease (IgG4/IgG ratio, storiform fibrosis, obliterative phlebitis) are met.
The recent recognition of the disease has enabled us to reclassify patients who we had previously diagnosed with “inflammatory pseudotumor”.6 The main objective of our study was to evaluate the prevalence of IgG4-RD in biopsies from patients sent to the pathology department of our hospital.
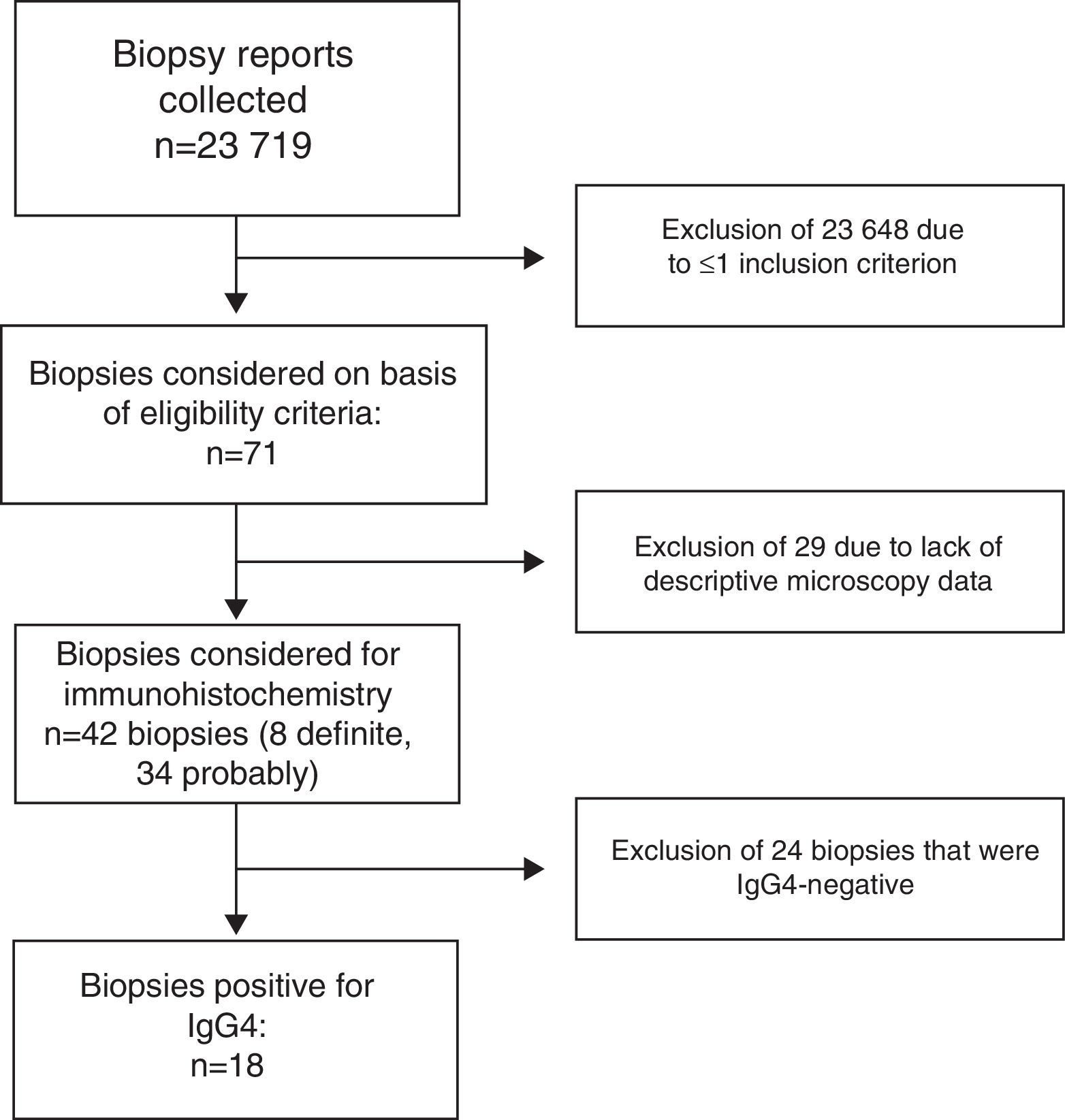
MethodsFor this retrospective clinical and histological study, we analyzed the biopsy reports issued by the pathology service of Hospital Central “Dr. Ignacio Morones Prieto” in San Luis Potosí, Mexico, from 7 January 2011 to 28 June 2013. The study was divided into 3 phases; the first involved the search for those reports in the pathology database that included data indicative of IgG4-RD8 (Fig. 1). At the time of this phase, none of the specimens had been examined by immunohistochemical staining for IgG4.

In the first phase, 2 of the researchers (DHV and TJP) carried out a manual search among the histology reports for all the specimens from January 2011 to June 2013, a total of 23,720 biopsies that exhibited the histological—not immunohistochemical—characteristics of IgG4-RD, such as: (a) nonspecific inflammatory response with lymphoplasmacytic infiltration; (b) inflammatory pseudotumors localized to any organ; (c) storiform fibrosis; and (d) obliterative phlebitis. Those specimens reported as neoplasms of any type or infections were excluded, as were all those for which the histological description was not available.
In the second phase, the biopsy findings were classified as probable or definite IgG4-RD according to the criteria proposed by Umehara et al.9 Probable disease was defined as the presence of 2 inclusion criteria, in which case, immunohistochemistry for IgG and IgG4 was performed, and definite disease as the presence of 3 or more inclusion criteria and IgG4 positivity, with an IgG4/IgG ratio ≥35%. The remaining specimens were excluded. We did a search for the clinical and demographic data of the patients whose biopsy results had indicated probable disease. Only 1 patient had undergone the determination of serum IgG4.
ImmunohistochemistryAn anti-IgG4 antibody (MRQ-44, Cell Marque) was used for this analysis. This antibody is available in prediluted form, which does not require reconstitution. (a) The block was deparaffinized and the antigen retrieved by means of heat-induced epitope retrieval (HIER) using Trilogy™ from Cell Marque; (b) the block was cut into sections of approximately 3μm; (c) after blocking, the antibody was incubated for 30min; (d) the HiDef amplifier for mouse was applied for 10min, followed by washing; (e) a polymer-based detection system was applied for 10min; and finally (f) chromogene was applied, followed by a 10-min incubation.
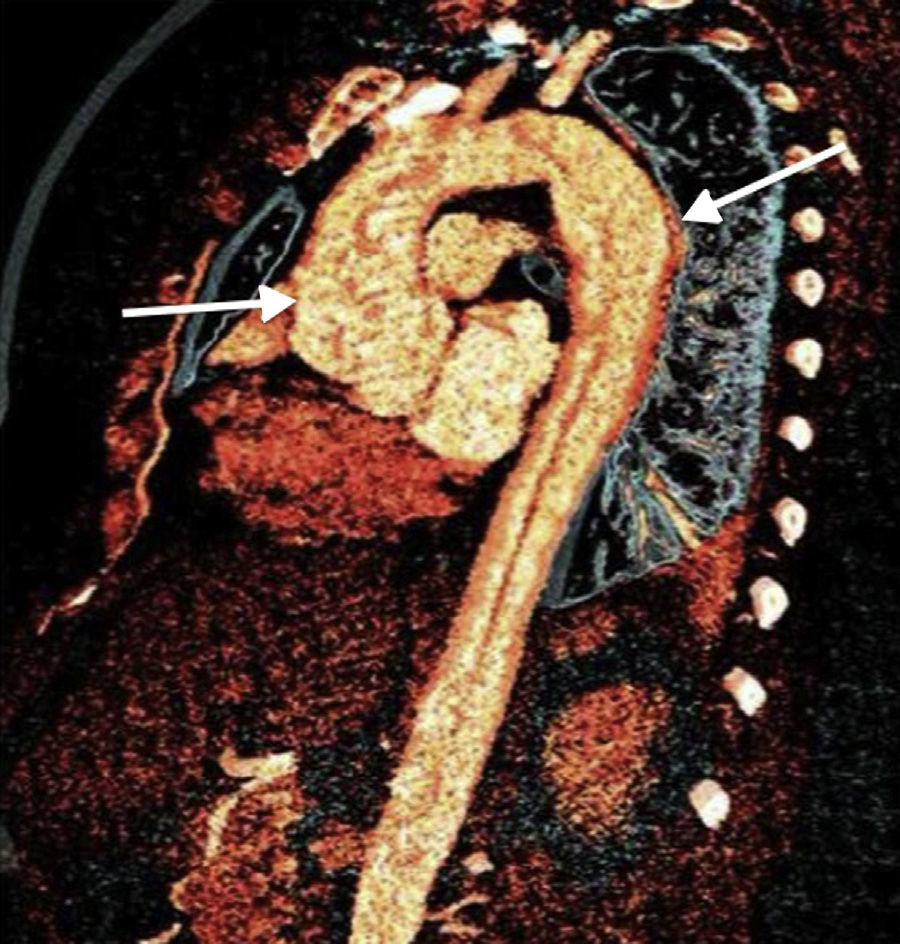
ResultsIn the first phase, we reviewed 23,720 biopsies. In the second phase, of 71 biopsies classified as probable, 8 were finally recorded as definite cases of IgG4-RD; the remainder of the specimens (n=63) were categorized as probable. The median age of the 3 women and 5 men whose specimens had been classified as definite cases was 45 (12–68) years. The diagnoses in the specimens with a definitive diagnosis of IgG4-RD referred for pathological study were (Fig. 2): aortitis (n=1), inflammatory pseudotumor of the lung (n=1), pancreatic tumor (n=1), pericarditis (n=1), lymphadenopathy under study (n=2), dacryoadenitis (n=1) and parotitis (n=1). The 2 patients with lymph node involvement were admitted to the hospital for fever of unknown origin and the patient with pancreatic tumor developed sclerosing cholangitis and salivary gland involvement. All were positive for IgG4 according to immunohistochemical analysis.

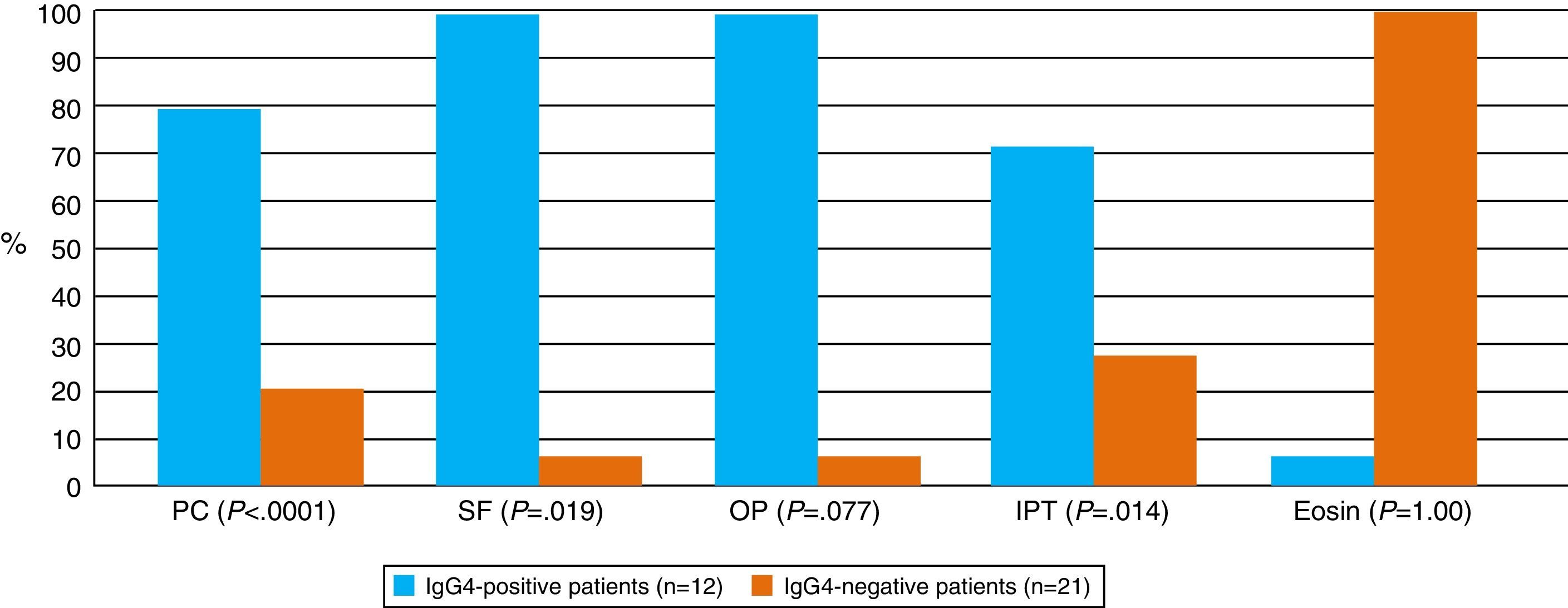
The probable group included 63 biopsies, which were reanalyzed; 29 were excluded because of insufficient microscopy data for diagnosis; the remaining biopsies were subjected to immunohistochemistry with IgG and IgG4. The pathological diagnoses prior to the immunohistochemical analysis of these biopsies are shown in Fig. 3. The IgG4+ specimens corresponded to: 5/17 cases of granulomatous mastitis, 1/1 case of chronic sclerosing dacryoadenitis, 2/9 cases of chronic sialoadenitis (1 associated with chronic pancreatitis), 1/2 cases of chronic thyroiditis, 1/1 case of chronic pancreatitis (Fig. 4). The percentage of IgG4+ plasma cells in the specimens ranged between 5% and 10% of the cells, in all the samples with an IgG4/IgG ratio >35%.

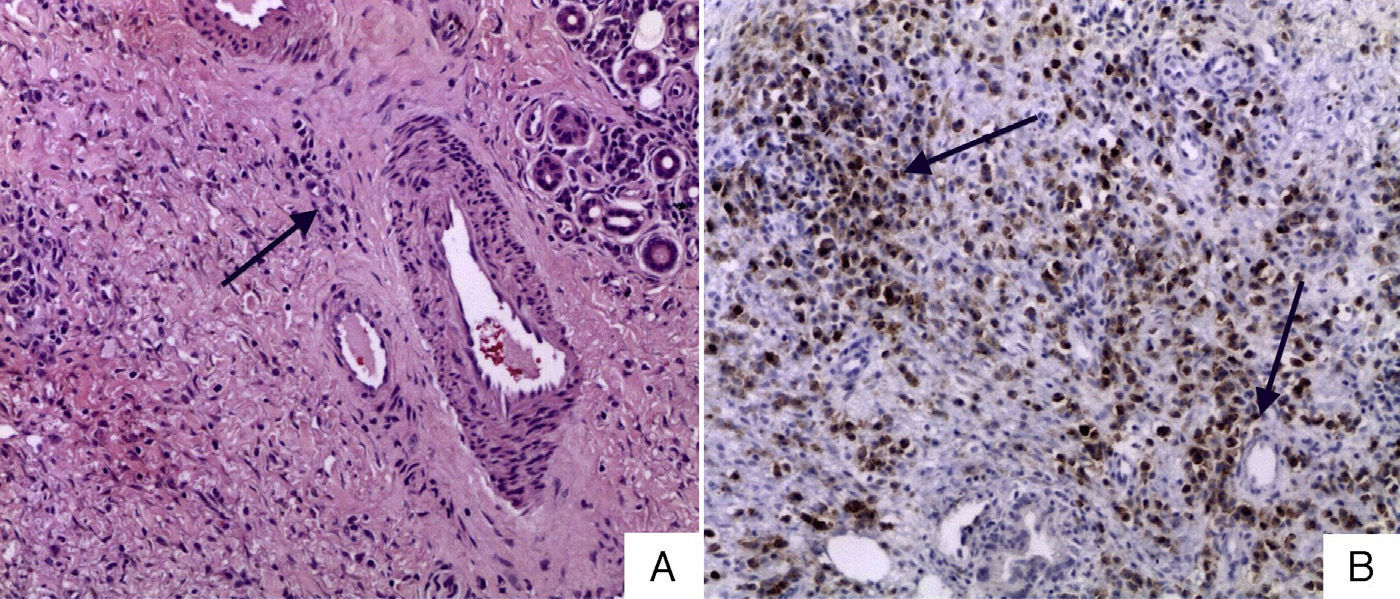
 Lacrimal gland stained with hematoxylin and eosin (40×): periglandular plasma cell infiltration with glandular distortion. (B) Immunohistochemistry of IgG4+ lacrimal gland, IgG4/IgG ratio >40%.")
In the evaluation of the definite and probable biopsies, we found a prevalence of IgG4-RD of 25.3%. It was interesting to note that the highest prevalence of positivity was observed among the specimens—classified as probable—in which the reference diagnosis was granulomatous mastitis.
Given that many of the biopsies were performed in an ambulatory setting and the fact that the pathology department is the state referral center for San Luis Potosí, it was not possible to obtain the complete clinical data for the majority of the patients.
DiscussionThe prevalence of IgG4-RD in Caucasian populations is described as being low, although there are no available registries of Hispanic or Latino populations. This circumstance highlights the importance of the present study, in which we found a prevalence of 24% in biopsies with histological changes that were indicative of probable, or were compatible with, IgG4-RD. Such a high prevalence is due to the fact that our hospital is a referral center and, as has been pointed out by different authors, the greatest prevalence of the disease is observed in university hospitals, where the incidence is 0.28–1.08 per 100 000 population, with 336–1300 new cases each year. These facts underline the importance of maintaining a high level of suspicion, not only clinical, but histological as well.10,11
Our study shows that, due to the lack of knowledge about the pathophysiology of IgG4-RD, these conditions are most probably underdiagnosed, and that, given the heterogeneity of the clinical signs, the final diagnosis should be based on the characteristic histopathological findings.
The reports in the literature dealing with the clinical picture of the disease stress the multiorgan association; the most common examples include salivary gland involvement and pancreatic, bile duct, lymph node and even renal involvement.12–15 Our findings contrast with these observations, given the higher prevalence of mammary gland involvement. This disease site has only been reported in a study carried out by Cheuk et al.,16 in which the authors, on evaluating the mammary gland biopsies with presence of pseudotumors, found a great abundance of IgG4-positive plasma cells. The scope of the present study was broader as we took into account all the histopathological diagnoses, not limiting ourselves to any one organ. Despite the fact that we do not provide serum IgG4 levels in our study, the histological findings, especially IgG4/IgG plasma cell ratio greater than 50% in the biopsy, the presence of storiform fibrosis or the presence of obliterative phlebitis, are representative, and may alone exhibit greater specificity.17,18
The retrospective nature of the study makes it difficult for us to categorically establish the diagnosis of IgG4-RD because of the lack of clinical and serological data of our patients, although, given their high specificity, the most important criteria for the diagnosis of diseases caused by IgG4 are the histological findings. This is not the case of the determination of serum IgG4 since, as reported by Ebbo et al.,7,15,19 elevated serum IgG4/IgG ratios were detected in infections and neoplasms, a fact that underscores the absence of specificity of this antibody in a number of clinical contexts. This circumstance also leads us to question the central role of IgG4, and ask whether, in some cases, the infiltrate and this immunoglobulin might be an epiphenomenon.
The diagnostic value of the histological changes in IgG4-RD is variable, taking into account the high sensitivity of the tests. Masaki et al.18 reported a low specificity (30%) and high sensitivity (99%) for different variables (e.g., an IgG4/IgG ratio of less than 10%). Thus, the diagnosis is based on the serum IgG4 level, the presence of storiform fibrosis, the plasma cell infiltrate and eosinophilia.20
The biological behavior of IgG4 is heterogeneous, since it has both anti-inflammatory properties, as has been observed in certain allergic or allergy-like diseases such as asthma,21 and pathological properties, through which it exerts a direct effect on different structures, as in pemphigus foliaceus, in which the antibody is directed against desmoglein 3.22 Although the behavior is clear in the preceding examples, the same cannot be said of other IgG4-RD in which, despite there being a number of reviews, it still is not clear whether the immunoglobulin is an epiphenomenon or plays a major role in the disease.1,2 The antigen that could trigger the disease is also unknown, despite a proteomic analysis in which a 13-kDa antigen was detected.23
ConclusionsOur report clearly stresses the high prevalence of IgG4-RD, pointing out that none of the biopsies initially subjected to histological analysis revealed evidence of the disease. Although we found the organ involvement characteristic of IgG4-RD, mammary gland involvement, defined as granulomatous mastitis, was highly prevalent.
Ethical DisclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of InterestThe authors declare they have no conflicts of interest.
Please cite this article as: Herrera van Oostdam DA, Piñón TJ, Martínez-Martínez MU, Oros-Ovalle C, Aléman-Sánchez N, Abud-Mendoza C. Enfermedades relacionadas con IgG4, diagnóstico histopatológico retrospectivo. Prevalencia en un hospital universitario. Reumatol Clin. 2015;11:335–339.


